Salway Travis, Rich Ashleigh J, Ferlatte Olivier, Gesink Dionne, Ross Lori E, Bränström Richard, Sadr Aida, Khan Syma, Grennan Troy, Shokoohi Mostafa, Brennan David J, Gilbert Mark
Faculty of Health Sciences, Simon Fraser University, Burnaby, Canada.
British Columbia Centre for Disease Control, Vancouver, Canada.
SSM Popul Health. 2022 Oct 27;20:101276. doi: 10.1016/j.ssmph.2022.101276. eCollection 2022 Dec.
Epidemiologic studies point to multiple health inequities among sexual minority people, but few studies have examined mortality. Some causes of death are more preventable than others, and access to prevention is theorized to follow patterns of access to social and material resources. The objective of this study is to compare estimates of preventable mortality between sexual minority (SM)-i.e., bisexual, lesbian, gay-and heterosexual adults in Canada.
A population-based retrospective cohort with 442,260 (unweighted N) Canadian adults, ages 18-59 years, was drawn from the Canadian Community Health Survey/Canadian Mortality Database linked database (2003-2017). The Rutstein preventability rating index was used to classify cause-specific mortality (low/high). Longitudinal analyses were conducted using Cox proportional hazards models.
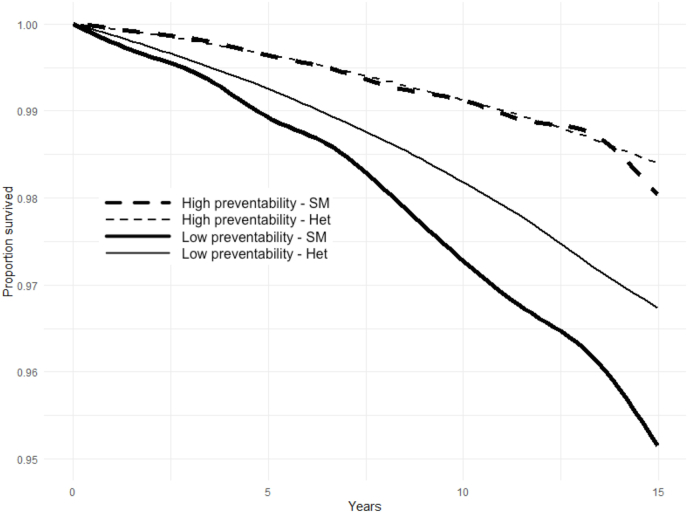
SM respondents had higher hazard of all-cause mortality (unadjusted hazard ratio [uHR] 1.28, 95% CI 1.06, 1.55). The uHR increased when the outcome was limited to highly-preventable causes of mortality (uHR 1.43, 95% CI 1.14, 1.80). The uHR further increased in sensitivity analyses using higher thresholds of the Rutstein index. SM respondents had higher hazard of cause-specific mortality for heart disease (uHR 1.53, 95% CI 1.03, 2.29), accidents (uHR 1.97, 95% CI 1.01, 3.86), HIV (uHR 75.69, 95% CI 18.77, 305.20), and suicide (uHR 2.22, 95% CI 0.93, 5.30) but not for cancer (uHR 0.86, 95% CI 0.60, 1.25). The adjusted HR (aHR) for highly-preventable mortality was not attenuated by adjustment for confounders (aHR 1.57, 95% CI 1.20, 2.05) but was reduced by adjustment for hypothesized mediators relating to access to social and material resources (marital status, children, income, education; aHR 1.11, 95% CI 0.78, 1.58).
Preventable mortality was elevated for SM Canadians compared to heterosexuals. Early and broad access to sexual minority-affirming primary and preventive healthcare should be expanded.
流行病学研究指出性少数群体存在多种健康不平等现象,但很少有研究调查死亡率。某些死因比其他死因更具可预防性,理论上预防措施的可及性遵循社会和物质资源的获取模式。本研究的目的是比较加拿大性少数群体(即双性恋、女同性恋、男同性恋)和异性恋成年人之间可预防性死亡率的估计值。
从加拿大社区健康调查/加拿大死亡率数据库链接数据库(2003 - 2017年)中抽取了一个基于人群的回顾性队列,其中包括442,260名(未加权N)年龄在18 - 59岁的加拿大成年人。使用鲁茨斯坦可预防性评级指数对特定原因死亡率进行分类(低/高)。使用Cox比例风险模型进行纵向分析。
性少数群体受访者的全因死亡率风险更高(未调整风险比[uHR]为1.28,95%置信区间为1.06,1.55)。当结果仅限于高度可预防的死因时,uHR增加(uHR为1.43,95%置信区间为1.14,1.80)。在使用鲁茨斯坦指数更高阈值的敏感性分析中,uHR进一步增加。性少数群体受访者患心脏病(uHR为1.53,95%置信区间为1.03,2.29)、事故(uHR为1.97,95%置信区间为1.01,3.86)、艾滋病毒(uHR为75.69,95%置信区间为18.77,305.20)和自杀(uHR为2.22,95%置信区间为0.93,5.30)的特定原因死亡率风险更高,但患癌症的风险不高(uHR为0.86,95%置信区间为0.60,1.25)。高度可预防性死亡率的调整后风险比(aHR)在对混杂因素进行调整后并未减弱(aHR为1.57,95%置信区间为1.20,2.05),但在对与社会和物质资源获取相关的假设中介因素(婚姻状况、子女、收入、教育程度)进行调整后降低了(aHR为1.11,95%置信区间为0.78,1.58)。
与异性恋者相比,加拿大性少数群体的可预防性死亡率有所升高。应扩大早期和广泛获取肯定性少数群体的初级和预防性医疗保健服务。