Al-Sunaidar Khalid Ahmad, Aziz Noorizan Abd, Hassan Yahaya, Jamshed Shazia, Sekar Mahendran
Department of Clinical Pharmacy and Pharmacy Practice, Faculty of Pharmacy and Health Sciences, Royal College of Medicine Perak, Universiti Kuala Lumpur, Ipoh 30450, Perak, Malaysia.
Department of Clinical Pharmacy, Faculty of Pharmacy, Universiti Teknologi MARA, Puncak Alam 42300, Selangor, Malaysia.
Trop Med Infect Dis. 2022 Nov 9;7(11):365. doi: 10.3390/tropicalmed7110365.
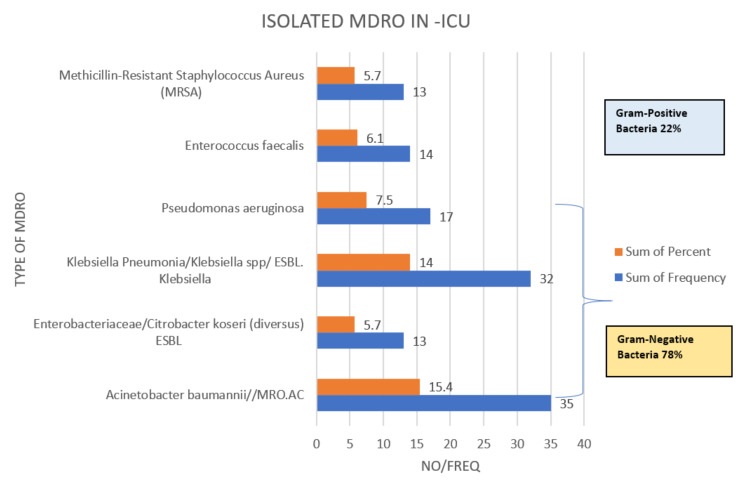
Background: Multi-drug resistance organisms (MDRO) often cause increased morbidity, mortality, and length of stays (LOS). However, there is uncertainty whether the infection of MDRO increase the morbidity, mortality, and ICU-LOS. Objective: This study was performed to determine the prevalence of MDRO in the ICU, the site of infection, and the association of MDRO or site of infection with mortality. The secondary outcome was determined by ascertaining the association of MDRO or site of infection with ICU-LOS. Methods: A retrospective cohort study was performed with adult sepsis patients in the ICU. Univariate and multivariate (MVA) logistic regression with cox regression modeling were performed to compute the association of MDRO with ICU mortality. MVA modelling was performed for ICU-LOS predictors. Results: Out of 228 patients, the isolated MDRO was 97 (42.5%), of which 78% were Gram-negative bacteria. The mortality rate among those with MDRO was 85 (37.3%). The hospital acquired infection (HAI) was a significant predictor for ICU-LOS in univariate linear regression (R2 = 0.034, p = 0.005). In MVA linear regression, both Enterococcus faecalis infection and Acinetobacter baumannii (AC)-MDRO were predictors for ICU-LOS with (R2 = 0.478, p < 0.05). In the univariate cox regression, only the infection with AC-MDRO was a risk factor for ICU-mortality with [HR = 1.802 (95% CI: 1.2−2.706; p = 0.005)]. Conclusions: Identifying risk factors for MDRO addresses the appropriate administration of empirical antibiotics and allows to effectively control the source of infection, which would reduce mortality and ICU-LOS. The usage of broad-spectrum antibiotics should be limited to those with substantial risk factors for acquiring MDRO.
多重耐药菌(MDRO)常导致发病率、死亡率增加以及住院时间延长。然而,MDRO感染是否会增加发病率、死亡率和重症监护病房住院时间(ICU-LOS)尚不确定。目的:本研究旨在确定重症监护病房中MDRO的患病率、感染部位,以及MDRO或感染部位与死亡率之间的关联。次要结局通过确定MDRO或感染部位与ICU-LOS之间的关联来确定。方法:对重症监护病房的成年脓毒症患者进行回顾性队列研究。采用单因素和多因素(MVA)逻辑回归及Cox回归模型来计算MDRO与ICU死亡率之间的关联。对ICU-LOS预测因素进行MVA建模。结果:在228例患者中,分离出的MDRO为97例(42.5%),其中78%为革兰氏阴性菌。MDRO患者的死亡率为85例(37.3%)。在单因素线性回归中,医院获得性感染(HAI)是ICU-LOS的显著预测因素(R2 = 0.034,p = 0.005)。在MVA线性回归中,粪肠球菌感染和鲍曼不动杆菌(AC)-MDRO均为ICU-LOS的预测因素(R2 = 0.478,p < 0.05)。在单因素Cox回归中,仅AC-MDRO感染是ICU死亡率的危险因素,[风险比(HR)= 1.802(95%置信区间:1.2 - 2.7);p = 0.005]。结论:识别MDRO的危险因素有助于合理使用经验性抗生素,并有效控制感染源,从而降低死亡率和ICU-LOS。广谱抗生素的使用应仅限于那些有大量获得MDRO风险因素的患者。