Rader Benjamin, Astley Christina M, Sewalk Kara, Delamater Paul L, Cordiano Kathryn, Wronski Laura, Rivera Jessica Malaty, Hallberg Kai, Pera Megan F, Cantor Jonathan, Whaley Christopher M, Bravata Dena M, Lee Leslie, Patel Anita, Brownstein John S
Computational Epidemiology Lab, Boston Children's Hospital, Boston, MA, USA.
Department of Epidemiology, Boston University School of Public Health, Boston, MA, USA.
Commun Med (Lond). 2022 Nov 10;2(1):141. doi: 10.1038/s43856-022-00183-8.
COVID-19 vaccine distribution is at risk of further propagating the inequities of COVID-19, which in the United States (US) has disproportionately impacted the elderly, people of color, and the medically vulnerable. We sought to measure if the disparities seen in the geographic distribution of other COVID-19 healthcare resources were also present during the initial rollout of the COVID-19 vaccine.
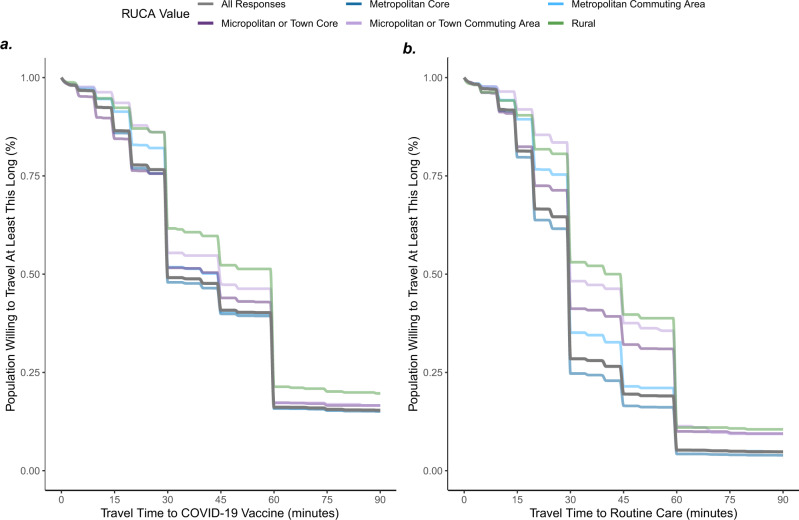
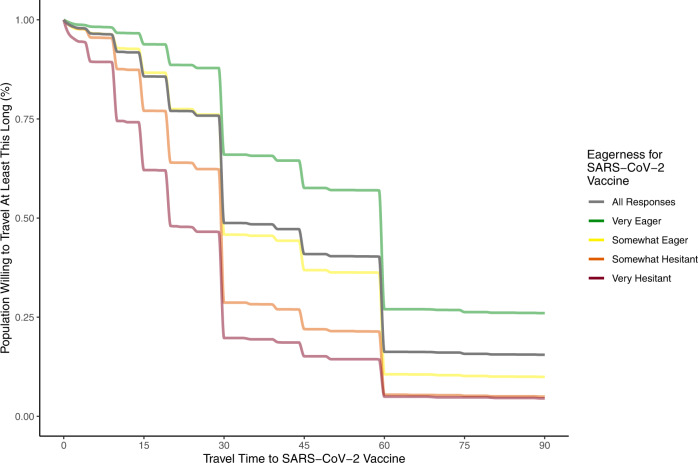
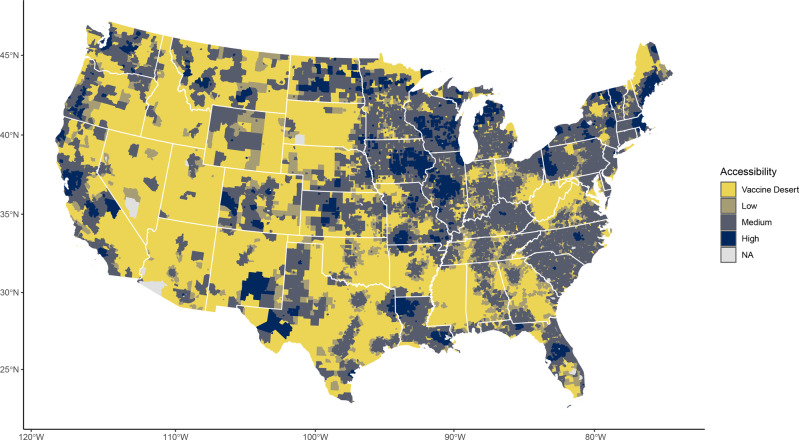
Using a comprehensive COVID-19 vaccine database (VaccineFinder), we built an empirically parameterized spatial model of access to essential resources that incorporated vaccine supply, time-willing-to-travel for vaccination, and previous vaccination across the US. We then identified vaccine deserts-US Census tracts with localized, geographic barriers to vaccine-associated herd immunity. We link our model results with Census data and two high-resolution surveys to understand the distribution and determinates of spatially accessibility to the COVID-19 vaccine.
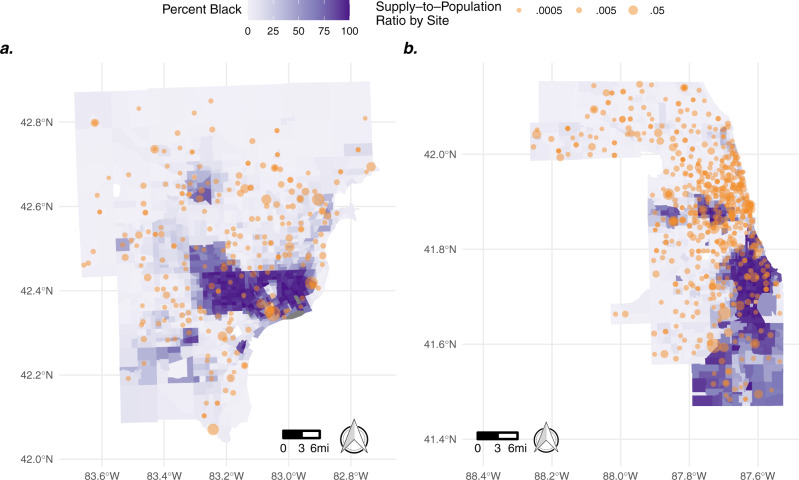
We find that in early 2021, vaccine deserts were home to over 30 million people, >10% of the US population. Vaccine deserts were concentrated in rural locations and communities with a higher percentage of medically vulnerable populations. We also find that in locations of similar urbanicity, early vaccination distribution disadvantaged neighborhoods with more people of color and older aged residents.
Given sufficient vaccine supply, data-driven vaccine distribution to vaccine deserts may improve immunization rates and help control COVID-19.
新冠病毒病(COVID-19)疫苗的分发有进一步加剧COVID-19不平等现象的风险,在美国,这种不平等现象对老年人、有色人种和医疗弱势群体的影响尤为严重。我们试图衡量在COVID-19疫苗首次推广期间,其他COVID-19医疗资源地理分布中所看到的差异是否也存在。
利用一个全面的COVID-19疫苗数据库(VaccineFinder),我们构建了一个经验参数化的基本资源获取空间模型,该模型纳入了疫苗供应、接种疫苗的时间意愿以及美国各地以前的接种情况。然后,我们确定了疫苗荒漠——美国人口普查区中存在与疫苗相关的群体免疫的局部地理障碍。我们将模型结果与人口普查数据和两项高分辨率调查联系起来,以了解COVID-19疫苗空间可及性的分布和决定因素。
我们发现,在2021年初,疫苗荒漠地区居住着超过3000万人,占美国人口的10%以上。疫苗荒漠集中在农村地区以及医疗弱势群体比例较高的社区。我们还发现,在城市化程度相似的地区,早期疫苗接种分布对有色人种和老年居民较多的社区不利。
在有足够疫苗供应的情况下,以数据驱动向疫苗荒漠地区分发疫苗可能会提高免疫率,并有助于控制COVID-19。