Division of Clinical Pharmacy, University of California, San Diego, Skaggs School of Pharmacy and Pharmaceutical Sciences, La Jolla, California, United States of America.
West Health Policy Center, Washington, DC, United States of America.
PLoS Med. 2022 Jul 28;19(7):e1004069. doi: 10.1371/journal.pmed.1004069. eCollection 2022 Jul.
The US Centers for Disease Control and Prevention has repeatedly called for Coronavirus Disease 2019 (COVID-19) vaccine equity. The objective our study was to measure equity in the early distribution of COVID-19 vaccines to healthcare facilities across the US. Specifically, we tested whether the likelihood of a healthcare facility administering COVID-19 vaccines in May 2021 differed by county-level racial composition and degree of urbanicity.
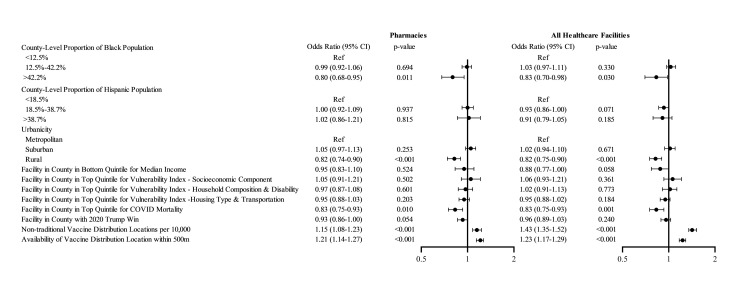
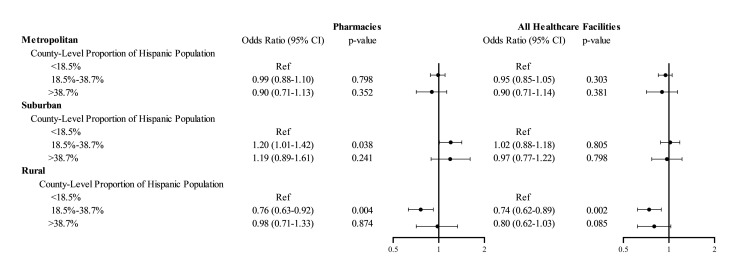
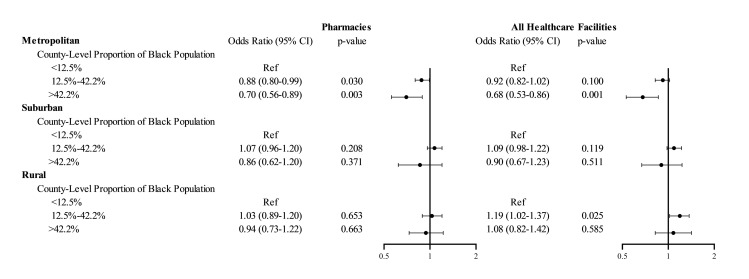
The outcome was whether an eligible vaccination facility actually administered COVID-19 vaccines as of May 2021, and was defined by spatially matching locations of eligible and actual COVID-19 vaccine administration locations. The outcome was regressed against county-level measures for racial/ethnic composition, urbanicity, income, social vulnerability index, COVID-19 mortality, 2020 election results, and availability of nontraditional vaccination locations using generalized estimating equations. Across the US, 61.4% of eligible healthcare facilities and 76.0% of eligible pharmacies provided COVID-19 vaccinations as of May 2021. Facilities in counties with >42.2% non-Hispanic Black population (i.e., > 95th county percentile of Black race composition) were less likely to serve as COVID-19 vaccine administration locations compared to facilities in counties with <12.5% non-Hispanic Black population (i.e., lower than US average), with OR 0.83; 95% CI, 0.70 to 0.98, p = 0.030. Location of a facility in a rural county (OR 0.82; 95% CI, 0.75 to 0.90, p < 0.001, versus metropolitan county) or in a county in the top quintile of COVID-19 mortality (OR 0.83; 95% CI, 0.75 to 0.93, p = 0.001, versus bottom 4 quintiles) was associated with decreased odds of serving as a COVID-19 vaccine administration location. There was a significant interaction of urbanicity and racial/ethnic composition: In metropolitan counties, facilities in counties with >42.2% non-Hispanic Black population (i.e., >95th county percentile of Black race composition) had 32% (95% CI 14% to 47%, p = 0.001) lower odds of serving as COVID administration facility compared to facilities in counties with below US average Black population. This association between Black composition and odds of a facility serving as vaccine administration facility was not observed in rural or suburban counties. In rural counties, facilities in counties with above US average Hispanic population had 26% (95% CI 11% to 38%, p = 0.002) lower odds of serving as vaccine administration facility compared to facilities in counties with below US average Hispanic population. This association between Hispanic ethnicity and odds of a facility serving as vaccine administration facility was not observed in metropolitan or suburban counties. Our analyses did not include nontraditional vaccination sites and are based on data as of May 2021, thus they represent the early distribution of COVID-19 vaccines. Our results based on this cross-sectional analysis may not be generalizable to later phases of the COVID-19 vaccine distribution process.
Healthcare facilities in counties with higher Black composition, in rural areas, and in hardest-hit communities were less likely to serve as COVID-19 vaccine administration locations in May 2021. The lower uptake of COVID-19 vaccinations among minority populations and rural areas has been attributed to vaccine hesitancy; however, decreased access to vaccination sites may be an additional overlooked barrier.
美国疾病控制与预防中心(Centers for Disease Control and Prevention)多次呼吁实现 2019 年冠状病毒病(COVID-19)疫苗公平分配。本研究旨在衡量 COVID-19 疫苗在 2021 年 5 月期间向美国各地医疗保健机构早期分配的公平性。具体来说,我们检验了在 2021 年 5 月,一个有条件接种疫苗的医疗保健机构进行 COVID-19 疫苗接种的可能性是否因县一级的种族构成和城市化程度而有所不同。
我们将是否有合格的接种点实际进行了 COVID-19 疫苗接种作为结果,并通过将合格和实际 COVID-19 疫苗接种点的地理位置相匹配来定义。利用广义估计方程,将县一级的种族/族裔构成、城市化程度、收入、社会脆弱性指数、COVID-19 死亡率、2020 年选举结果以及非传统疫苗接种点的可用性等因素纳入回归分析。在美国,截至 2021 年 5 月,有 61.4%的合格医疗保健机构和 76.0%的合格药房提供了 COVID-19 疫苗接种。与人口中非西班牙裔黑人比例低于 12.5%(即低于美国平均水平)的县相比,人口中非西班牙裔黑人比例超过 42.2%(即第 95 个黑人种族构成县百分位数以上)的县的医疗设施更不可能成为 COVID-19 疫苗接种点,比值比(OR)为 0.83;95%置信区间(CI)为 0.70 至 0.98,p=0.030。与大都市区县相比,位于农村县(OR 0.82;95%CI,0.75 至 0.90,p<0.001)或 COVID-19 死亡率处于最高五分位数(OR 0.83;95%CI,0.75 至 0.93,p=0.001)的县的医疗设施更不可能成为 COVID-19 疫苗接种点。城市化程度和种族/族裔构成之间存在显著的交互作用:在大都市区县,人口中非西班牙裔黑人比例超过 42.2%(即第 95 个黑人种族构成县百分位数以上)的县的医疗设施成为 COVID 管理设施的可能性比人口中非西班牙裔黑人比例低于美国平均水平的县低 32%(95%CI,14%至 47%,p=0.001)。这种黑人构成与设施成为疫苗接种点之间的关联在农村或郊区县并不存在。在农村县,人口中西班牙裔比例高于美国平均水平的县的医疗设施成为疫苗接种点的可能性比人口中西班牙裔比例低于美国平均水平的县低 26%(95%CI,11%至 38%,p=0.002)。这种医疗设施成为疫苗接种点的可能性与西班牙裔族裔之间的关联在大都市区或郊区县并不存在。我们的分析不包括非传统疫苗接种点,并且基于截至 2021 年 5 月的数据,因此代表了 COVID-19 疫苗的早期分配情况。我们基于这一横断面分析的结果可能不适用于 COVID-19 疫苗分配过程的后期阶段。
2021 年 5 月,黑人比例较高、位于农村地区和受灾最严重社区的医疗保健机构更不可能成为 COVID-19 疫苗接种点。少数族裔和农村地区 COVID-19 疫苗接种率较低归因于疫苗犹豫;然而,接种点获取途径减少可能是另一个被忽视的障碍。