Israel Defense Forces, Medical Corps, Jerusalem, Israel.
Clalit Health Services, Jerusalem, Israel.
Isr J Health Policy Res. 2022 Nov 10;11(1):38. doi: 10.1186/s13584-022-00542-9.
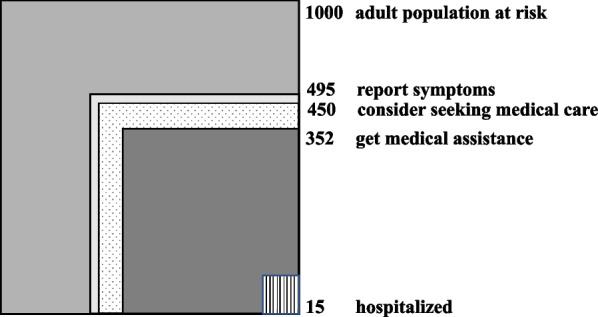
The Ecology of medical care was first published in 1961. The graphical square model showed that 75% of the population in the US and England experience a feeling of illness during a given month, 25% seek medical help and only one percent are hospitalized. In 2001, Green and colleagues found the same findings despite the many changes that occurred over the past decades. The frequency of illness, the desire for assistance and the frequency of seeking and getting medical assistance may differ in different populations due to cultural, economic, social, demographic background and local Health policy. This work describes the ecology of medical care consumption in Israel for the first time and examines the socio-demographic effects on consumption.
This is a Nationwide cross-sectional study. A telephone survey was conducted among a representative sample of the adult population (> 15 years) in Israel. Subjective morbidity rate in the preceding month, the rate of those considering medical assistance and those who got assistance were calculated. Correlation between socio-demographic variables and patterns of morbidity and medical care consumption was examined using a t-test and chi square for continuous quantitative and categorical variables. Logistic regression was used for multivariate analysis.
A total of 1862 people participated; 49.5% reported having symptoms in the previous month, 45% considered seeking medical advice, 35.2% sought out medical assistance and only 1.5% were hospitalized. The vast majority chose to contact their family physician (58%) and the primary care setting provided their needs in 80% of the cases; Subjective morbidity and medical care consumption differed significantly between Israeli Jews and Arabs. Gaps in the availability of medical services were observed as residents of the periphery forewent medical services significantly more than others (OR = 1.42, p = 0.026).
Subjective morbidity is less common in Israel than in other countries, but paradoxically consumption of medical services is higher. An Israeli who feels ill will usually consider receiving assistance and will indeed receive assistance in most cases. However, a greater tendency to forego medical services in the periphery indicates barriers and inequality in the provision of health services. Different cultural perceptions, lack of knowledge and low accessibility to medical services in the periphery probably contribute to the contrast shown between low consumption of medical services and high prevalence of chronic illness in Arab society. The prevailing preference for family medicine and its ability to deal with most requests for assistance suggest that strengthening family medicine in the periphery may reduce those barriers and inequalities.
《医疗保健生态学》于 1961 年首次出版。图形方形模型显示,在美国和英国,75%的人口在给定的一个月内会感到不适,25%的人会寻求医疗帮助,只有 1%的人会住院。2001 年,Green 及其同事发现,尽管过去几十年发生了许多变化,但仍有同样的发现。由于文化、经济、社会、人口背景和当地卫生政策的不同,疾病的发生频率、寻求帮助的愿望以及寻求和获得医疗帮助的频率在不同人群中可能有所不同。这项工作首次描述了以色列医疗保健消费的生态,并研究了社会人口统计学对消费的影响。
这是一项全国性的横断面研究。在以色列成年人(>15 岁)中进行了一项代表性样本的电话调查。计算了前一个月的主观发病率、考虑寻求医疗帮助的人数和获得帮助的人数。使用 t 检验和卡方检验连续定量和分类变量,研究社会人口统计学变量与发病率和医疗保健消费模式之间的相关性。多变量分析采用逻辑回归。
共有 1862 人参与;49.5%的人报告在前一个月有症状,45%的人考虑寻求医疗建议,35.2%的人寻求医疗帮助,只有 1.5%的人住院。绝大多数人选择联系他们的家庭医生(58%),初级保健机构满足了 80%的需求;主观发病率和医疗保健消费在以色列犹太人(Jews)和阿拉伯人之间存在显著差异。观察到医疗服务提供方面的差距,因为边缘地区的居民明显比其他人更不愿意接受医疗服务(OR=1.42,p=0.026)。
与其他国家相比,以色列的主观发病率较低,但医疗服务的消费却较高。一个感到不适的以色列人通常会考虑接受帮助,而且在大多数情况下确实会得到帮助。然而,边缘地区更倾向于放弃医疗服务,表明在提供卫生服务方面存在障碍和不平等。不同的文化观念、缺乏知识以及边缘地区医疗服务的低可及性,可能导致阿拉伯社会中医疗服务低消费和慢性病高患病率之间的反差。家庭医学的普遍偏好及其处理大多数援助请求的能力表明,在边缘地区加强家庭医学可能会减少这些障碍和不平等。



