Klinik für Allgemein-, Viszeral-, Thorax- und Kinderchirurgie Kliniken Boeblingen, Boeblingen, Germany.
Institut für Pathologie der Ruhr-Universität Bochum, Bochum, Germany.
Br J Surg. 2022 Dec 13;110(1):98-105. doi: 10.1093/bjs/znac379.
Complete mesocolic excision (CME) for right colonic cancer is a more complex operation than standard right hemicolectomy but evidence to support its routine use is still limited. This prospective multicentre study evaluated the effect of CME on long-term survival in colorectal cancer centres in Germany (RESECTAT trial). The primary hypothesis was that 5-year disease-free survival would be higher after CME than non-CME surgery. A secondary hypothesis was that there would be improved survival of patients with a mesenteric area greater than 15 000 mm2.
Centres were asked to continue their current surgical practices. The surgery was classified as CME if the superior mesenteric vein was dissected; otherwise it was assumed that no CME had been performed. All specimens were shipped to one institution for pathological analysis and documentation. Clinical data were recorded in an established registry for quality assurance. The primary endpoint was 5-year overall survival for stages I-III. Multivariable adjustment for group allocation was planned. Using a primary hypothesis of an increase in disease-free survival from 60 to 70 per cent, a sample size of 662 patients was calculated with a 50 per cent anticipated drop-out rate.
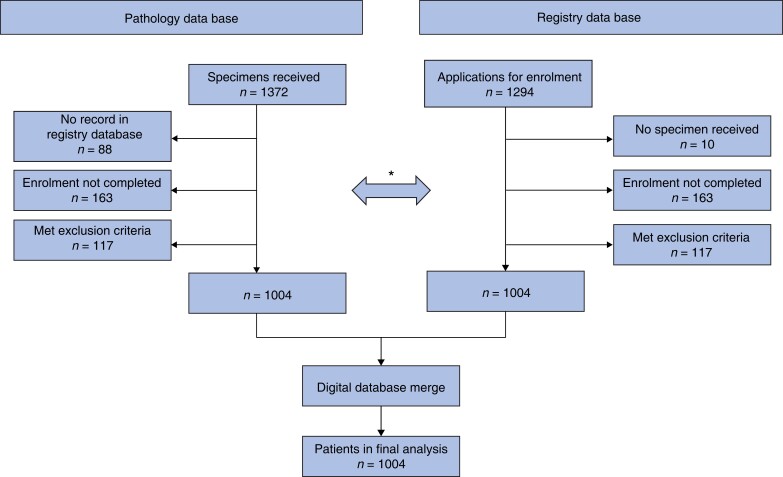
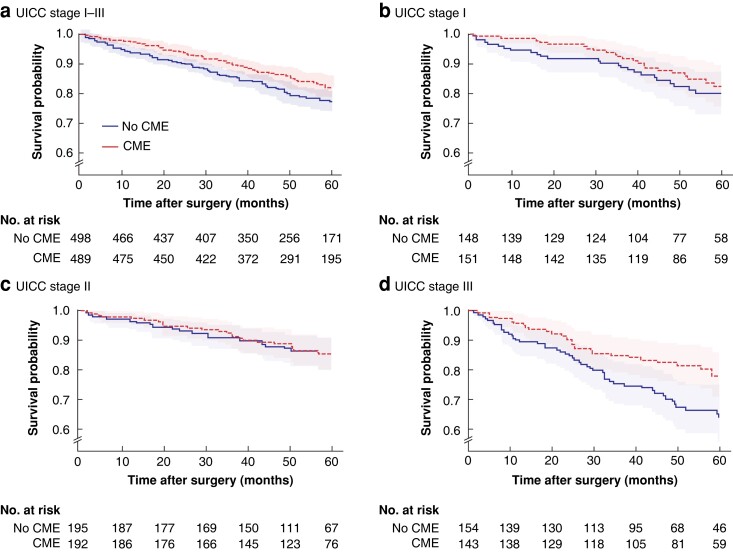
A total of 1004 patients from 53 centres were recruited for the final analysis (496 CME, 508 no CME). Most operations (88.4 per cent) were done by an open approach. Anastomotic leak occurred in 3.4 per cent in the CME and 1.8 per cent in the non-CME group. There were slightly more lymph nodes found in CME than non-CME specimens (mean 55.6 and 50.4 respectively). Positive central mesenteric nodes were detected more in non-CME than CME specimens (5.9 versus 4.0 per cent). One-fifth of patients had died at the time of study with recorded recurrences (63, 6.3 per cent), too few to calculate disease-free survival (the original primary outcome), so overall survival (not disease-specific) results are presented. Short-term and overall survival were similar in the CME and non-CME groups. Adjusted Cox regression indicated a possible benefit for overall survival with CME in stage III disease (HR 0.52, 95 per cent c.i. 0.31 to 0.85; P = 0.010) but less so for disease-free survival (HR 0.66; P = 0.068). The secondary outcome (15 000 mm2 mesenteric size) did not influence survival at any stage (removal of more mesentery did not alter survival).
No general benefit of CME could be established. The observation of better overall survival in stage III on unplanned exploratory analysis is of uncertain significance.
与标准右半结肠切除术相比,完整结肠系膜切除术(CME)治疗右半结肠癌的操作更为复杂,但支持其常规应用的证据仍然有限。这项前瞻性多中心研究在德国的结直肠癌中心评估了 CME 对长期生存的影响(RESECTAT 试验)。主要假设是 CME 后的无病生存率高于非 CME 手术。次要假设是肠系膜面积大于 15000mm2 的患者的生存率会提高。
要求各中心继续进行目前的手术治疗。如果肠系膜上静脉被解剖,则手术被归类为 CME;否则,假设未进行 CME。所有标本均运往一个机构进行病理分析和记录。临床数据记录在一个既定的登记处,以确保质量。主要终点是 I-III 期的 5 年总生存率。计划进行组分配的多变量调整。根据无病生存率从 60%增加到 70%的主要假设,预计有 662 例患者脱落,计算出的样本量为 662 例。
共招募了来自 53 个中心的 1004 名患者进行最终分析(496 名 CME,508 名非 CME)。大多数手术(88.4%)都是通过开放方法进行的。CME 组吻合口漏发生率为 3.4%,非 CME 组为 1.8%。CME 标本中的淋巴结数量略多于非 CME 标本(分别为 55.6 和 50.4 个)。非 CME 标本中检测到更多的中央肠系膜阳性淋巴结(分别为 5.9%和 4.0%)。研究时,1/5 的患者已经死亡并记录到复发(63 例,6.3%),复发人数太少,无法计算无病生存率(最初的主要结局),因此报告了总体生存率(非疾病特异性)结果。CME 组和非 CME 组的短期和总体生存率相似。调整后的 Cox 回归表明,CME 在 III 期疾病中可能对总体生存率有获益(HR 0.52,95%置信区间 0.31 至 0.85;P=0.010),但对无病生存率的获益较小(HR 0.66;P=0.068)。次要结局(肠系膜面积大于 15000mm2)在任何阶段都没有影响生存(切除更多的肠系膜并不能改变生存)。
不能确定 CME 有普遍获益。计划外探索性分析中观察到 III 期总体生存率更好的结果意义不确定。