IRCCS S. Maria Nascente - Fondazione Don Carlo Gnocchi ONLUS, Milan, Italy.
Intensive Cardiac Care Unit, Città della Salute e della Scienza di Torino, Torino, Italy.
Catheter Cardiovasc Interv. 2023 Jan;101(1):22-32. doi: 10.1002/ccd.30484. Epub 2022 Nov 15.
Cardiogenic shock (CS) includes several phenotypes with heterogenous hemodynamic features. Timely prognostication is warranted to identify patients requiring treatment escalation. We explored the association of the updated Society for Cardiovascular Angiography and Interventions (SCAI) stages classification with in-hospital mortality using a prospective national registry.
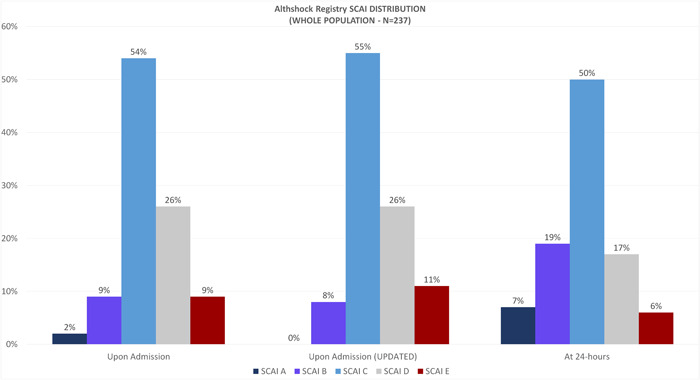
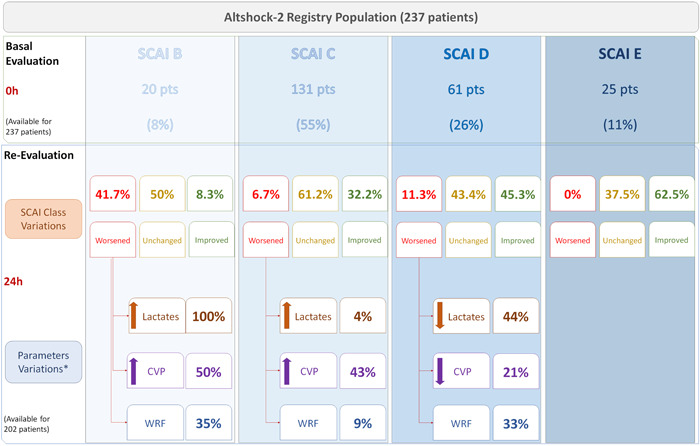
Between March 2020 and February 2022 the Altshock-2 Registry has included 237 patients with CS of all etiologies at 11 Italian Centers. Patients were classified according to their admission SCAI stage (assigned prospectively and independently updated according to the recently released version). In-hospital mortality was evaluated for association with both admission and 24-h SCAI stages.
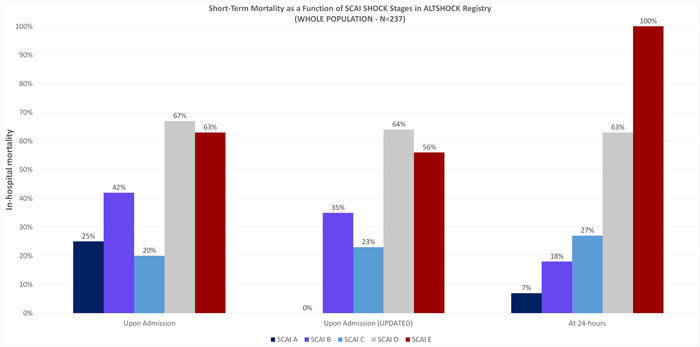
The overall in-hospital mortality was 38%. Of the 237 patients included and staged according to the updated SCAI classification, 20 (8%) had SCAI shock stage B, 131 (55%) SCAI stage C, 61 (26%) SCAI stage D and 25 (11%) SCAI stage E. In-hospital mortality stratified according to the SCAI classification at 24 h was 18% for patients in SCAI stage B, 27% for SCAI stage C, 63% for SCAI stage D and 100% for SCAI stage E. Both the revised SCAI stages on admission and at 24 h were associated with in-hospital mortality, but the classification potential slightly increased at 24-h. After adjusting for age, sex, lactate level, eGFR, CVP, inotropic score and mechanical circulatory support [MCS], SCAI classification at 24 h was an independent predictor of in-hospital mortality.
In the Altshock-2 registry the utility of SCAI shock stages to identify risk of in-hospital mortality increased at 24 h after admission. Escalation of treatment (either pharmacological or with MCS) should be tailored to achieve prompt clinical improvement within the first 24 h after admission. Registration: http://www.
gov; Unique identifier: NCT04295252.
心原性休克(CS)包括多种具有异质血流动力学特征的表型。及时预测有助于识别需要治疗升级的患者。我们使用前瞻性国家登记处探讨了更新的心血管血管造影和介入学会(SCAI)分期分类与院内死亡率的关系。
在 2020 年 3 月至 2022 年 2 月期间,Altshock-2 登记处纳入了来自意大利 11 个中心的各种病因 CS 的 237 名患者。患者根据入院时的 SCAI 分期进行分类(前瞻性分配并根据最近发布的版本独立更新)。评估入院时和 24 小时 SCAI 分期与院内死亡率的关系。
总的院内死亡率为 38%。在根据更新的 SCAI 分类纳入并分期的 237 名患者中,20 名(8%)为 SCAI 休克 B 期,131 名(55%)为 SCAI 期 C,61 名(26%)为 SCAI 期 D,25 名(11%)为 SCAI 期 E。根据 SCAI 分类在 24 小时分层的院内死亡率为 SCAI 期 B 为 18%,SCAI 期 C 为 27%,SCAI 期 D 为 63%,SCAI 期 E 为 100%。入院时和 24 小时修订的 SCAI 分期均与院内死亡率相关,但 24 小时后分类能力略有增加。在校正年龄、性别、乳酸水平、eGFR、CVP、正性肌力评分和机械循环支持 [MCS] 后,24 小时 SCAI 分类是院内死亡率的独立预测因子。
在 Altshock-2 登记处,入院后 24 小时 SCAI 休克分期用于识别院内死亡率风险的效用增加。应根据需要调整治疗(药物或 MCS),以在入院后 24 小时内实现快速临床改善。注册:http://www.clinicaltrials.gov;独特标识符:NCT04295252。