Roslin Institute, University of Edinburgh, Edinburgh, UK.
These authors contributed equally to this work.
Eur Respir Rev. 2022 Nov 15;31(166). doi: 10.1183/16000617.0030-2022. Print 2022 Dec 31.
To assess the safety and efficacy of extracorporeal carbon dioxide removal (ECCOR) standard care in patients with acute hypoxaemic respiratory failure (AHRF).
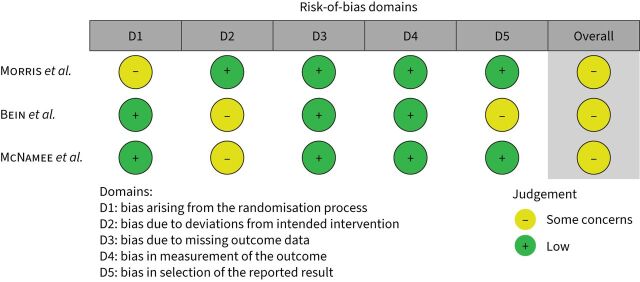
MEDLINE, Embase and clinical trial registries were searched from 1994 to 31 December 2021. We included randomised controlled trials (RCTs) and observational studies. Pairs of reviewers independently extracted data and assessed the risk of bias. The primary outcome was mortality. Secondary outcomes included ventilator-free days, length of stay, safety and adverse events and physiological changes. As a primary analysis, we performed a meta-analysis of mortality until day 30 using a Bayesian random effects model. We then performed a trial sequential analysis of RCTs.
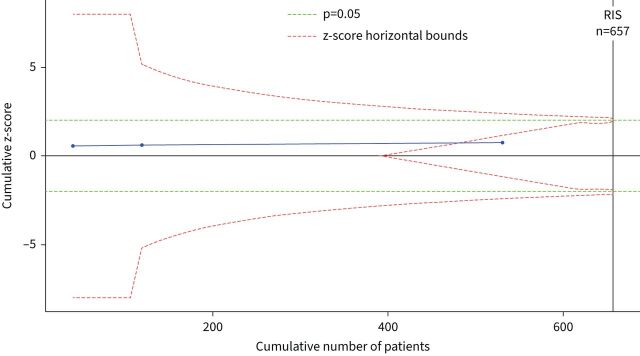
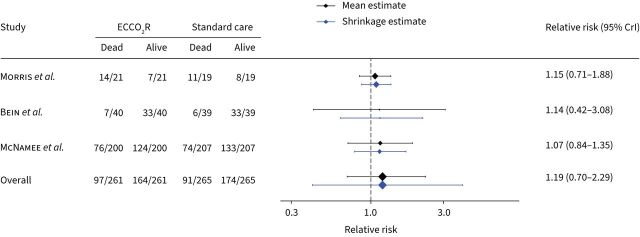
21 studies met inclusion criteria: three RCTs, enrolling 531 patients, and 18 observational studies. In a pooled analysis of RCTs, the posterior probability of increased mortality with the use of ECCOR was 73% (relative risk 1.19, 95% credible interval 0.70-2.29). There was substantial heterogeneity in the reporting of safety and adverse events. However, the incidence of extra and intracranial haemorrhage was higher (relative risk 3.00, 95% credible interval 0.41-20.51) among those randomised to ECCOR. Current trials have accumulated 80.8% of the diversity-adjusted required information size and the lack of effect reaches futility for a 10% absolute risk reduction in mortality.
The use of ECCOR in patients with AHRF is not associated with improvements in clinical outcomes. Furthermore, it is likely that further trials of ECCOR aiming to achieve an absolute risk reduction in mortality of ≥10% are futile.
评估体外二氧化碳去除(ECCOR)标准治疗在急性低氧性呼吸衰竭(AHRF)患者中的安全性和疗效。
从 1994 年至 2021 年 12 月 31 日,我们检索了 MEDLINE、Embase 和临床试验注册库。我们纳入了随机对照试验(RCT)和观察性研究。由两名审查员独立提取数据并评估偏倚风险。主要结局为死亡率。次要结局包括无呼吸机天数、住院时间、安全性和不良事件以及生理变化。作为主要分析,我们使用贝叶斯随机效应模型对第 30 天前的死亡率进行了荟萃分析。然后,我们对 RCT 进行了试验序贯分析。
有 21 项研究符合纳入标准:3 项 RCT,纳入 531 例患者,18 项观察性研究。在 RCT 的汇总分析中,使用 ECCOR 增加死亡率的后验概率为 73%(相对风险 1.19,95%可信区间 0.70-2.29)。在安全性和不良事件的报告中存在很大的异质性。然而,随机分配到 ECCOR 组的患者发生额外和颅内出血的风险更高(相对风险 3.00,95%可信区间 0.41-20.51)。目前的试验已经积累了 80.8%的多样性调整所需信息量,而且缺乏效果表明,死亡率降低 10%的绝对风险降低达到无效。
在 AHRF 患者中使用 ECCOR 与临床结局的改善无关。此外,进一步试验 ECCOR 旨在实现死亡率降低 10%以上的绝对风险降低可能是无效的。