Wiesel Ory, Kaufman Daniel, Caplan-Shaw Caralee, Shaw Jason
The Cardiovascular Institute, Division of Thoracic Surgery, Baruch-Padeh Medical Center of the North, Poriya, Israel.
The Faculty of Medicine in the Galilee, Bar-Ilan University, Ramat Gan, Israel.
J Thorac Dis. 2022 Oct;14(10):3727-3736. doi: 10.21037/jtd-22-183.
Accurate mediastinal staging of lung cancer patients is critical for determining appropriate treatment. Mediastinoscopy and endobronchial ultrasound (EBUS)-guided transbronchial needle aspiration are the most commonly utilized techniques. Limited data exist on training and practice trends among thoracic surgeons. We aimed to determine training and practice patterns and find whether there is a paradigm shift in mediastinal staging after the introduction of EBUS into practice among thoracic surgeons in the United States.
28-question survey was constructed querying demographic, training, and practice patterns with mediastinoscopy and EBUS and was sent to practicing thoracic surgeons in the United States. Descriptive statistics were used to summarize quantitative data.
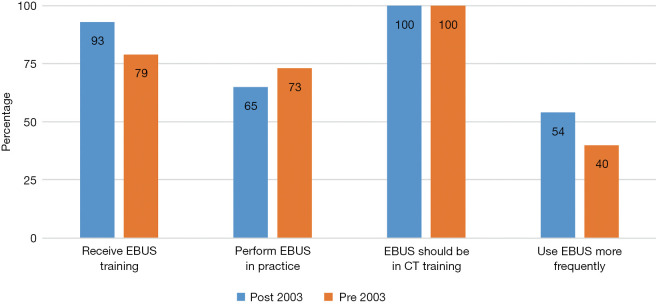
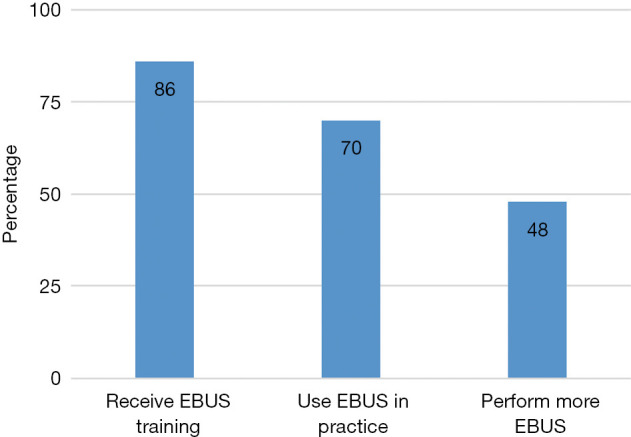
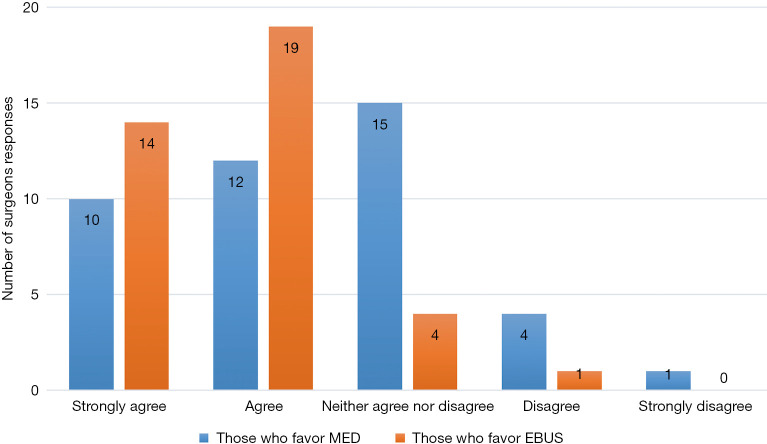
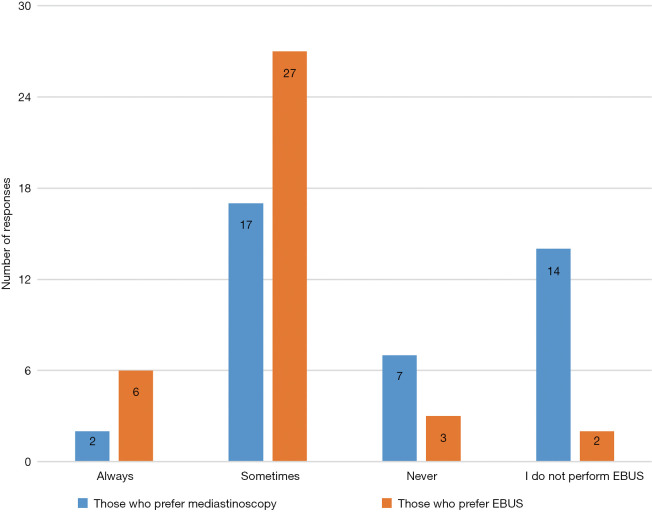
Ninety-eight responded with a 93% completion rate. Eighty-seven percent of respondents received training in EBUS and 70% perform EBUS routinely. All respondents believe EBUS should be incorporated into thoracic surgery training curriculums. Majority of those who prefer EBUS feel EBUS is safer than mediastinoscopy, allows access to lymph nodes stations or lesions inaccessible by mediastinoscopy and prefer EBUS to avoid re-do mediastinoscopy and in irradiated mediastinum. Majority of those who prefer mediastinoscopy reported they perform more accurate staging compared to EBUS, that mediastinoscopy is more accurate in diagnosing lymphoma or sarcoidosis and that frozen section can be done at the same interval as resection. Among surgeons who prefer EBUS, 94% biopsy 3 or more lymph node stations, 86% routinely biopsy hilar (N1) nodes while 8% never biopsy N1 nodes. Of surgeons who prefer mediastinoscopy. Ninety-seven percent biopsy 3 or more lymph node stations, only 27% routinely biopsy N1 nodes and 70% never biopsy N1 nodes.
EBUS is used frequently by thoracic surgeons in their practice for mediastinal staging. Methods of obtaining proficiency in EBUS widely varied among surgeons. In addition to mediastinoscopy, dedicated EBUS training should be incorporated into thoracic surgery training curriculums.
肺癌患者准确的纵隔分期对于确定合适的治疗方案至关重要。纵隔镜检查和支气管内超声(EBUS)引导下经支气管针吸活检是最常用的技术。关于胸外科医生的培训和实践趋势的数据有限。我们旨在确定培训和实践模式,并了解在美国胸外科医生将EBUS应用于实践后,纵隔分期是否存在模式转变。
构建了一份包含28个问题的调查问卷,询问有关纵隔镜检查和EBUS的人口统计学、培训及实践模式,并发送给美国执业胸外科医生。使用描述性统计来总结定量数据。
98人回复,完成率为93%。87%的受访者接受过EBUS培训,70%常规进行EBUS操作。所有受访者都认为EBUS应纳入胸外科培训课程中。大多数更喜欢EBUS的人认为EBUS比纵隔镜检查更安全,能够检查纵隔镜无法到达的淋巴结站或病变,并且更喜欢EBUS以避免再次进行纵隔镜检查以及用于照射后的纵隔。大多数更喜欢纵隔镜检查的人报告称,与EBUS相比,他们进行的分期更准确,纵隔镜检查在诊断淋巴瘤或结节病方面更准确,并且可以在与切除相同的间隔时间进行冰冻切片检查。在更喜欢EBUS 的外科医生中,94%对3个或更多淋巴结站进行活检,86%常规对肺门(N1)淋巴结进行活检,而8%从未对N1淋巴结进行活检。在更喜欢纵隔镜检查的外科医生中,97%对3个或更多淋巴结站进行活检,只有27%常规对N1淋巴结进行活检,70%从未对N1淋巴结进行活检结论:胸外科医生在实践中经常使用EBUS进行纵隔分期。外科医生获得EBUS熟练程度的方法差异很大。除纵隔镜检查外,应将专门的EBUS培训纳入胸外科培训课程中。