National Institutes for Quantum Science and Technology, Quantum Life and Medical Science Directorate, Institute for Quantum Medical Science, Inage-ku, Chiba 263-8555, Japan.
Department of Radiation Oncology, Tata Medical Center, 14, MAR(E-W), DH Block (Newtown), Action Area I, Newtown, Kolkata, West Bengal 700160, India.
J Radiat Res. 2023 Jan 20;64(1):162-170. doi: 10.1093/jrr/rrac074.
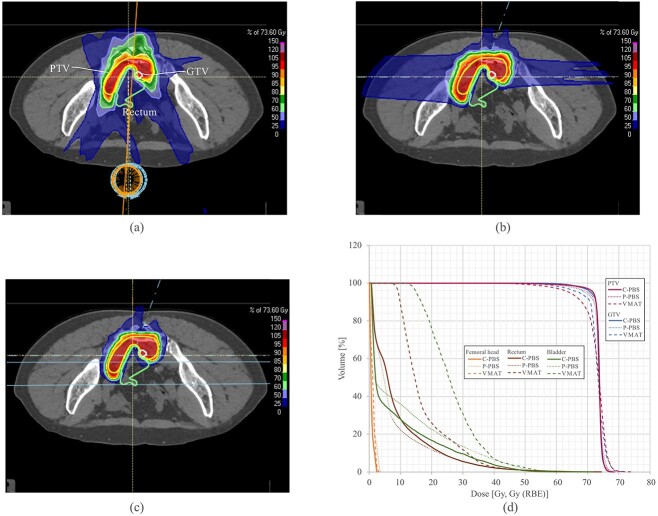
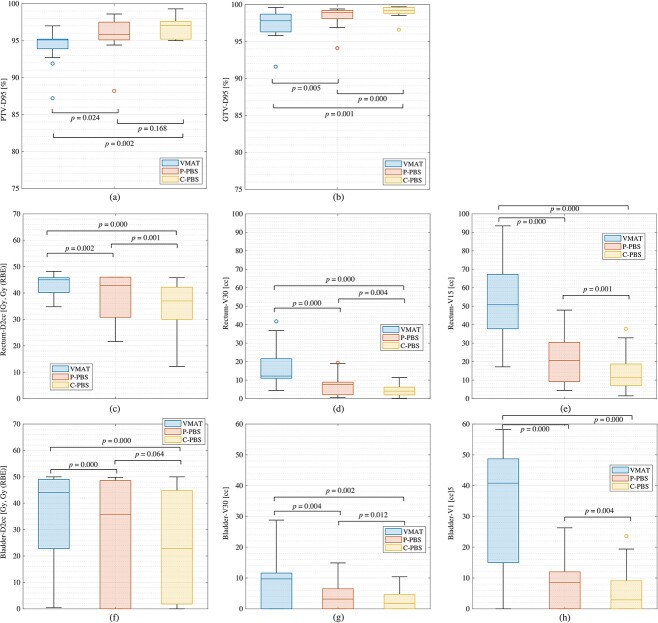
We compared the dose distributions of carbon-ion pencil beam scanning (C-PBS), proton pencil beam scanning (P-PBS) and Volumetric Modulated Arc Therapy (VMAT) for locally recurrent rectal cancer. The C-PBS treatment planning computed tomography (CT) data sets of 10 locally recurrent rectal cancer cases were randomly selected. Three treatment plans were created using identical prescribed doses. The beam angles for C-PBS and P-PBS were identical. Dosimetry, including the dose received by 95% of the planning target volume (PTV) (D95%), dose to the 2 cc receiving the maximum dose (D2cc), organ at risk (OAR) volume receiving > 15Gy (V15) and > 30Gy (V30), was evaluated. Statistical significance was assessed using the Wilcoxon signed-rank test. Mean PTV-D95% values were > 95% of the volume for P-PBS and C-PBS, whereas that for VMAT was 94.3%. However, PTV-D95% values in P-PBS and VMAT were < 95% in five and two cases, respectively, due to the OAR dose reduction. V30 and V15 to the rectum/intestine for C-PBS (V30 = 4.2 ± 3.2 cc, V15 = 13.8 ± 10.6 cc) and P-PBS (V30 = 7.3 ± 5.6 cc, V15 = 21.3 ± 13.5 cc) were significantly lower than those for VMAT (V30 = 17.1 ± 10.6 cc, V15 = 55.2 ± 28.6 cc). Bladder-V30 values with P-PBS/C-PBS (3.9 ± 4.8 Gy(RBE)/3.0 ± 4.0 Gy(RBE)) were significantly lower than those with VMAT (7.9 ± 8.1 Gy). C-PBS provided superior dose conformation and lower OAR doses compared with P-PBS and VMAT. C-PBS may be the best choice for cases in which VMAT and P-PBS cannot satisfy dose constraints. C-PBS could be another choice for cases in which VMAT and P-PBS cannot satisfy dose constraints, thereby avoiding surgical resection.
我们比较了碳离子铅笔束扫描(C-PBS)、质子铅笔束扫描(P-PBS)和容积旋转调强放疗(VMAT)治疗局部复发性直肠癌的剂量分布。随机选择了 10 例局部复发性直肠癌的 C-PBS 治疗计划 CT 数据集。使用相同的规定剂量创建了三个治疗计划。C-PBS 和 P-PBS 的射束角度相同。评估了包括 95%计划靶区(PTV)接受剂量(D95%)、2cc 接受最大剂量(D2cc)、接受>15Gy(V15)和>30Gy(V30)的器官受量(OAR)体积在内的剂量学。使用 Wilcoxon 符号秩检验评估统计学意义。P-PBS 和 C-PBS 的 PTV-D95%值均大于 95%的体积,而 VMAT 为 94.3%。然而,由于 OAR 剂量减少,P-PBS 和 VMAT 中有 5 例和 2 例 PTV-D95%值<95%。C-PBS(V30=4.2±3.2cc,V15=13.8±10.6cc)和 P-PBS(V30=7.3±5.6cc,V15=21.3±13.5cc)的直肠/肠 V30 和 V15 明显低于 VMAT(V30=17.1±10.6cc,V15=55.2±28.6cc)。P-PBS/C-PBS 的膀胱 V30 值(3.9±4.8Gy(RBE)/3.0±4.0Gy(RBE))明显低于 VMAT(7.9±8.1Gy)。C-PBS 与 P-PBS 和 VMAT 相比,提供了更好的剂量一致性和更低的 OAR 剂量。C-PBS 可能是 VMAT 和 P-PBS 不能满足剂量限制的情况下的最佳选择。C-PBS 也可以作为不能满足剂量限制的情况下的另一种选择,从而避免手术切除。