Cornejo Rodrigo A, Montoya Jorge, Gajardo Abraham I J, Graf Jerónimo, Alegría Leyla, Baghetti Romyna, Irarrázaval Anita, Santis César, Pavez Nicolás, Leighton Sofía, Tomicic Vinko, Morales Daniel, Ruiz Carolina, Navarrete Pablo, Vargas Patricio, Gálvez Roberto, Espinosa Victoria, Lazo Marioli, Pérez-Araos Rodrigo A, Garay Osvaldo, Sepúlveda Patrick, Martinez Edgardo, Bruhn Alejandro
Unidad de Pacientes Críticos, Departamento de Medicina, Hospital Clínico Universidad de Chile, Dr. Carlos Lorca Tobar 999, 2º Piso, Independencia, Santiago, Chile.
Center of Acute Respiratory Critical Illness (ARCI), Santiago, Chile.
Ann Intensive Care. 2022 Nov 28;12(1):109. doi: 10.1186/s13613-022-01082-w.
Prone positioning is currently applied in time-limited daily sessions up to 24 h which determines that most patients require several sessions. Although longer prone sessions have been reported, there is scarce evidence about the feasibility and safety of such approach. We analyzed feasibility and safety of a continuous prolonged prone positioning strategy implemented nationwide, in a large cohort of COVID-19 patients in Chile.
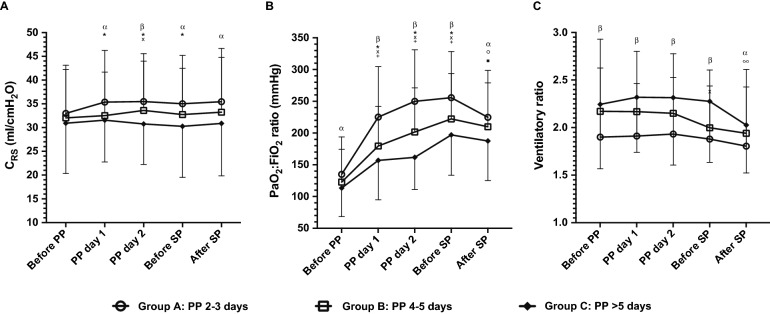
Retrospective cohort study of mechanically ventilated COVID-19 patients with moderate-to-severe acute respiratory distress syndrome (ARDS), conducted in 15 Intensive Care Units, which adhered to a national protocol of continuous prone sessions ≥ 48 h and until PaO:FiO increased above 200 mm Hg. The number and extension of prone sessions were registered, along with relevant physiologic data and adverse events related to prone positioning. The cohort was stratified according to the first prone session duration: Group A, 2-3 days; Group B, 4-5 days; and Group C, > 5 days. Multivariable regression analyses were performed to assess whether the duration of prone sessions could impact safety.
We included 417 patients who required a first prone session of 4 (3-5) days, of whom 318 (76.3%) received only one session. During the first prone session the main adverse event was grade 1-2 pressure sores in 97 (23.9%) patients; severe adverse events were infrequent with 17 non-scheduled extubations (4.2%). 90-day mortality was 36.2%. Ninety-eight patients (24%) were classified as group C; they exhibited a more severe ARDS at baseline, as reflected by lower PaO:FiO ratio and higher ventilatory ratio, and had a higher rate of pressure sores (44%) and higher 90-day mortality (48%). However, after adjustment for severity and several relevant confounders, prone session duration was not associated with mortality or pressure sores.
Nationwide implementation of a continuous prolonged prone positioning strategy for COVID-19 ARDS patients was feasible. Minor pressure sores were frequent but within the ranges previously described, while severe adverse events were infrequent. The duration of prone session did not have an adverse effect on safety.
目前俯卧位通气每天限时应用,最长24小时,这意味着大多数患者需要进行多次。尽管有报道称俯卧时间更长,但关于这种方法的可行性和安全性的证据很少。我们分析了在智利一大群新冠肺炎患者中全国范围内实施的持续延长俯卧位策略的可行性和安全性。
对15个重症监护病房中患有中重度急性呼吸窘迫综合征(ARDS)的机械通气新冠肺炎患者进行回顾性队列研究,这些患者遵循全国性方案,进行持续俯卧≥48小时,直至动脉血氧分压与吸入氧浓度比值(PaO₂:FiO₂)升至200 mmHg以上。记录俯卧的次数和时长,以及相关生理数据和与俯卧位通气相关的不良事件。根据首次俯卧位通气的持续时间对队列进行分层:A组,2 - 3天;B组,4 - 5天;C组,>5天。进行多变量回归分析以评估俯卧位通气的持续时间是否会影响安全性。
我们纳入了417例首次俯卧位通气需4(3 - 5)天的患者,其中318例(76.3%)仅进行了一次俯卧位通气。在首次俯卧位通气期间,主要不良事件是97例(23.9%)患者出现1 - 2级压疮;严重不良事件较少见,有17例非计划性拔管(4.2%)。90天死亡率为36.2%。98例患者(24%)被归类为C组;他们在基线时ARDS更严重,表现为较低的PaO₂:FiO₂比值和较高的通气比,压疮发生率更高(44%),90天死亡率更高(48%)。然而,在对严重程度和几个相关混杂因素进行调整后,俯卧位通气的持续时间与死亡率或压疮无关。
在全国范围内对新冠肺炎ARDS患者实施持续延长俯卧位策略是可行的。轻度压疮很常见,但在先前描述的范围内,而严重不良事件很少见。俯卧位通气的持续时间对安全性没有不利影响。