DMU ESPRIT, Service de Médecine Intensive Réanimation, AP-HP, Hôpital Louis Mourier, 92700, Colombes, France.
Department of Epidemiology, Biostatistics and Clinical Research, AP-HP, Hôpital Bichat, 75018, Paris, France.
Crit Care. 2022 Jul 8;26(1):208. doi: 10.1186/s13054-022-04081-2.
During the COVID-19 pandemic, many more patients were turned prone than before, resulting in a considerable increase in workload. Whether extending duration of prone position may be beneficial has received little attention. We report here benefits and detriments of a strategy of extended prone positioning duration for COVID-19-related acute respiratory distress syndrome (ARDS).
A eetrospective, monocentric, study was performed on intensive care unit patients with COVID-19-related ARDS who required tracheal intubation and who have been treated with at least one session of prone position of duration greater or equal to 24 h. When prone positioning sessions were initiated, patients were kept prone for a period that covered two nights. Data regarding the incidence of pressure injury and ventilation parameters were collected retrospectively on medical and nurse files of charts. The primary outcome was the occurrence of pressure injury of stage ≥ II during the ICU stay.
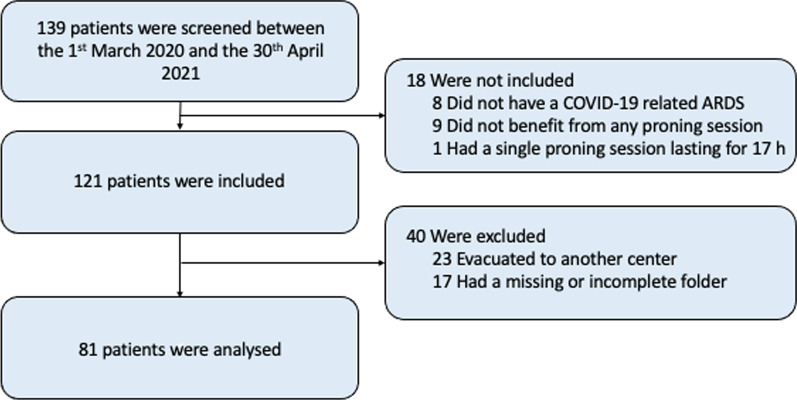
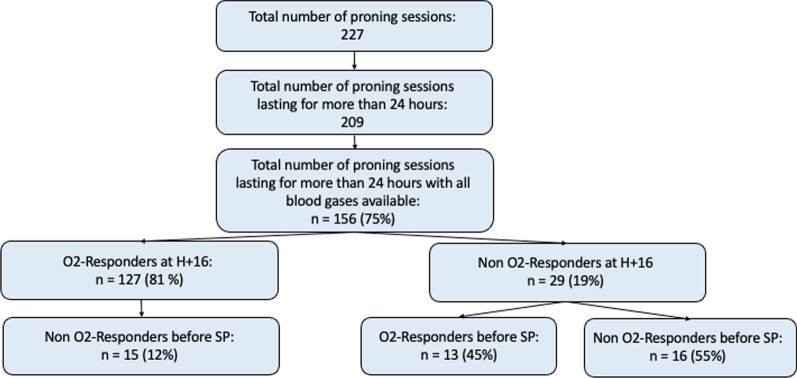
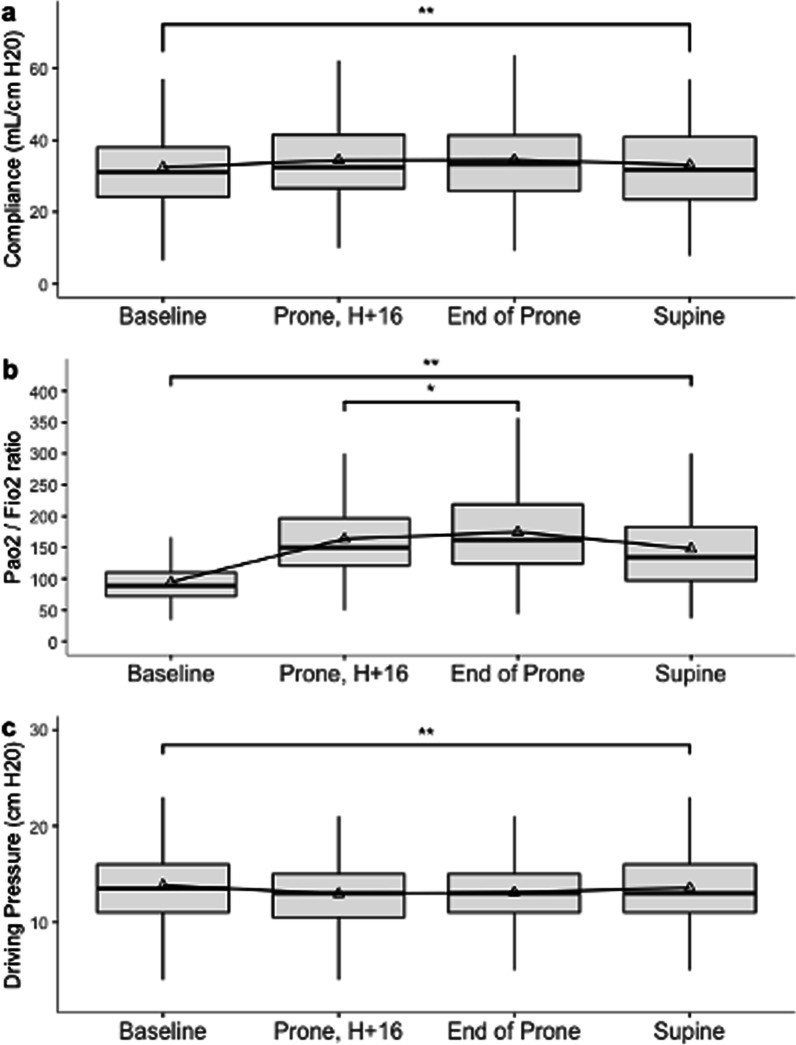
For the 81 patients included, the median duration of prone positioning sessions was 39 h [interquartile range (IQR) 34-42]. The cumulated incidence of stage ≥ II pressure injuries was 26% [95% CI 17-37] and 2.5% [95% CI 0.3-8.8] for stages III/IV pressure injuries. Patients were submitted to a median of 2 sessions [IQR 1-4] and for 213 (94%) prone positioning sessions, patients were turned over to supine position during daytime, i.e., between 9 AM and 6 PM. This increased duration was associated with additional increase in oxygenation after 16 h with the PaO/FiO ratio increasing from 150 mmHg [IQR 121-196] at H+ 16 to 162 mmHg [IQR 124-221] before being turned back to supine (p = 0.017).
In patients with extended duration of prone position up to 39 h, cumulative incidence for stage ≥ II pressure injuries was 26%, with 25%, 2.5%, and 0% for stage II, III, and IV, respectively. Oxygenation continued to increase significantly beyond the standard 16-h duration. Our results may have significant impact on intensive care unit staffing and patients' respiratory conditions.
Institutional review board 00006477 of HUPNVS, Université Paris Cité, APHP, with the reference: CER-2021-102, obtained on October 11th 2021. Registered at Clinicaltrials (NCT05124197).
在 COVID-19 大流行期间,需要俯卧位通气的患者比以往任何时候都多,这导致工作量显著增加。俯卧位时间延长是否有益,目前还没有得到太多关注。我们在此报告 COVID-19 相关急性呼吸窘迫综合征(ARDS)患者延长俯卧位时间的策略的益处和危害。
这是一项回顾性、单中心研究,纳入了需要气管插管且至少接受过一次持续时间超过 24 小时的俯卧位通气的 COVID-19 相关 ARDS 患者。当开始俯卧位通气时,患者的俯卧位时间为两个晚上。通过查阅病历和护理记录来收集压力性损伤发生率和通气参数的数据。主要结局是 ICU 住院期间发生 II 期及以上压力性损伤的情况。
共纳入 81 例患者,俯卧位通气时间的中位数为 39 小时[四分位距(IQR)34-42]。累积 II 期及以上压力性损伤发生率为 26%[95%CI 17-37],III/IV 期压力性损伤发生率为 2.5%[95%CI 0.3-8.8]。患者接受了中位数为 2 次[IQR 1-4]的俯卧位通气,213 次[94%]俯卧位通气期间,患者在白天(即上午 9 点至下午 6 点)被翻转为仰卧位。这种时间的延长与 16 小时后氧合的进一步增加有关,即 PaO/FiO 比值从俯卧位开始后的 16 小时的 150mmHg[IQR 121-196]增加到翻转为仰卧位前的 162mmHg[IQR 124-221](p=0.017)。
在俯卧位时间延长至 39 小时的患者中,II 期及以上压力性损伤的累积发生率为 26%,其中 II 期、III 期和 IV 期的发生率分别为 25%、2.5%和 0%。氧合作用在超过标准 16 小时后继续显著增加。我们的结果可能对重症监护病房的人员配备和患者的呼吸状况产生重大影响。
巴黎第五大学巴黎笛卡尔大学 HUPNVS 的机构审查委员会 00006477,参考号:CER-2021-102,于 2021 年 10 月 11 日获得。在 Clinicaltrials(NCT05124197)注册。