Division of Epidemiology & Community Health, School of Public Health, University of Minnesota, Minneapolis, MN.
M Health Fairview, University of Minnesota, Minneapolis, MN.
Chest. 2023 Apr;163(4):942-952. doi: 10.1016/j.chest.2022.11.028. Epub 2022 Nov 26.
OSA has been linked to microaspiration, systemic inflammation, and suboptimal immune function.
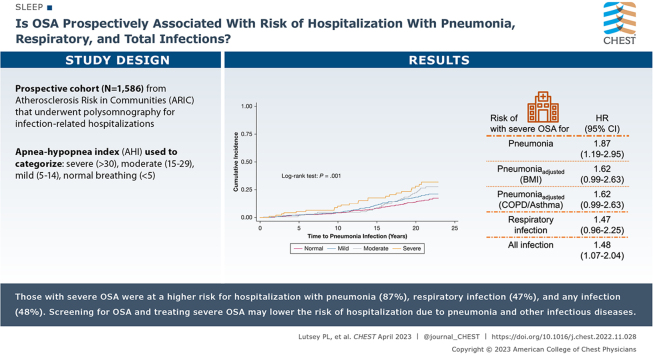
Is OSA prospectively associated with risk of hospitalization for pneumonia, respiratory, and total infections?
Prospective cohort. Participants in the Atherosclerosis Risk in Communities (ARIC) study (N = 1,586) underwent polysomnography in 1996-1998 and were followed up through 2018 for infection-related hospitalizations. The apnea-hypopnea index (AHI; events/h) was used to categorize participants as having severe OSA (≥ 30), moderate OSA (15-29), mild OSA (5-14), or a normal breathing pattern (< 5). Cox regression was used to calculate hazard ratios (HRs) and 95% CIs.
ARIC participants were on average 62.7 (SD = 5.5) years of age, and 52.8% were female. Severe OSA was present in 6.0%, moderate OSA in 12.7%, mild OSA in 30.0%, and normal breathing in 51.3%. A total of 253 hospitalizations with pneumonia occurred over a median 20.4 (max, 22.9) years' follow-up. Participants with severe OSA were at 1.87 times (95% CI, 1.19-2.95) higher risk of hospitalization with pneumonia compared with those with a normal breathing pattern after adjustment for demographics and lifestyle behaviors. Results were attenuated modestly after adjustment for BMI (1.62 [0.99-2.63]), and prevalent asthma and COPD (1.62 [0.99-2.63]). A similar pattern existed for hospitalization with respiratory infection and composite infection (demographic and behavior-adjusted HRs: 1.47 [0.96-2.25] and 1.48 [1.07-2.04], respectively).
Severe OSA was associated with increased risk of hospitalizations with pneumonia in this community-based cohort. OSA patients may benefit from more aggressive efforts to prevent pneumonia and other infectious conditions.
阻塞性睡眠呼吸暂停(OSA)与微吸入、全身炎症和免疫功能低下有关。
OSA 是否与肺炎、呼吸道和总感染的住院风险呈前瞻性相关?
前瞻性队列研究。参与动脉粥样硬化风险社区(ARIC)研究的 1586 名参与者在 1996-1998 年接受了多导睡眠图检查,并在 2018 年之前因感染相关住院进行了随访。使用呼吸暂停低通气指数(AHI;事件/小时)将参与者分为严重 OSA(≥ 30)、中度 OSA(15-29)、轻度 OSA(5-14)或正常呼吸模式(< 5)。使用 Cox 回归计算风险比(HR)和 95%置信区间(CI)。
ARIC 参与者的平均年龄为 62.7(标准差=5.5)岁,52.8%为女性。严重 OSA 占 6.0%,中度 OSA 占 12.7%,轻度 OSA 占 30.0%,正常呼吸占 51.3%。在中位 20.4(最长 22.9)年的随访期间,共发生 253 例肺炎住院。在调整人口统计学和生活方式行为后,与正常呼吸模式相比,严重 OSA 参与者患肺炎的住院风险高 1.87 倍(95%CI,1.19-2.95)。调整 BMI(1.62[0.99-2.63])和现患哮喘和 COPD(1.62[0.99-2.63])后,结果略有减弱。对于呼吸道感染和复合感染的住院治疗,也存在类似的模式(人口统计学和行为调整后的 HR:1.47[0.96-2.25]和 1.48[1.07-2.04])。
在这项基于社区的队列研究中,严重 OSA 与肺炎住院风险增加相关。OSA 患者可能受益于更积极地预防肺炎和其他感染性疾病。