Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Endocrine Research Center, Research Institute for Endocrine Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Cardiovasc Diabetol. 2022 Dec 3;21(1):267. doi: 10.1186/s12933-022-01709-z.
We aimed to assess the gender-specific impact of 3-year changes in fasting plasma glucose (FPG) status on the risk of all-cause, cardiovascular (CV), and cancer mortality in individuals without type 2 diabetes (T2DM) during an 18-year follow-up.
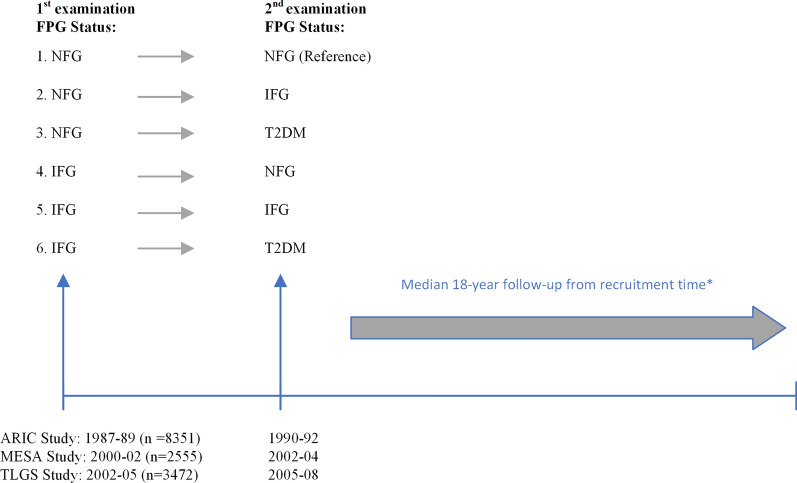
The study population included 14,378 participants aged 30-60 years (8272 women) from three population-based cohort studies, including Atherosclerosis Risk in Communities, Multi-Ethnic Study of Atherosclerosis, and Tehran Lipid and Glucose Study. Subjects were classified into six categories based on the approximately three-year changes in FPG status: (1) normal FPG (NFG) to NFG (reference category); (2) NFG to impaired fasting glucose (IFG) (i.e., 126 > FPG ≥ 100 mg/dl); (3) NFG to T2DM; (4) IFG to NFG; (5) IFG to IFG; (6) IFG to T2DM. Multivariable stratified Cox regression, adjusting for age, body mass index (BMI), BMI-Change, smoking status, hypertension, and hypercholesterolemia was used to estimate hazard ratios (HRs (95% CI)) for all-cause and cause-specific mortality events. Women-to-men ratios of HRs (RHRs) for each category were also estimated.
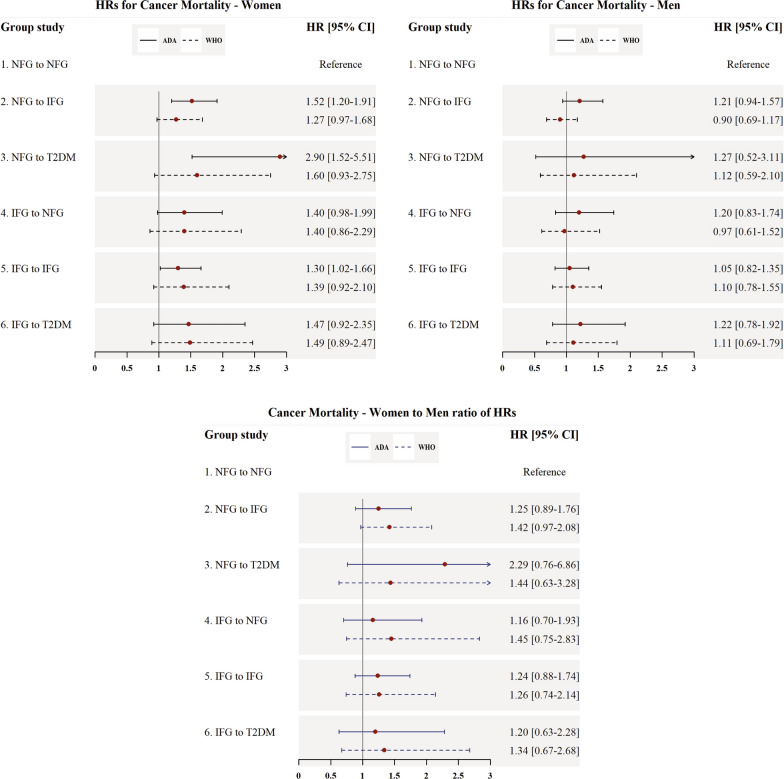
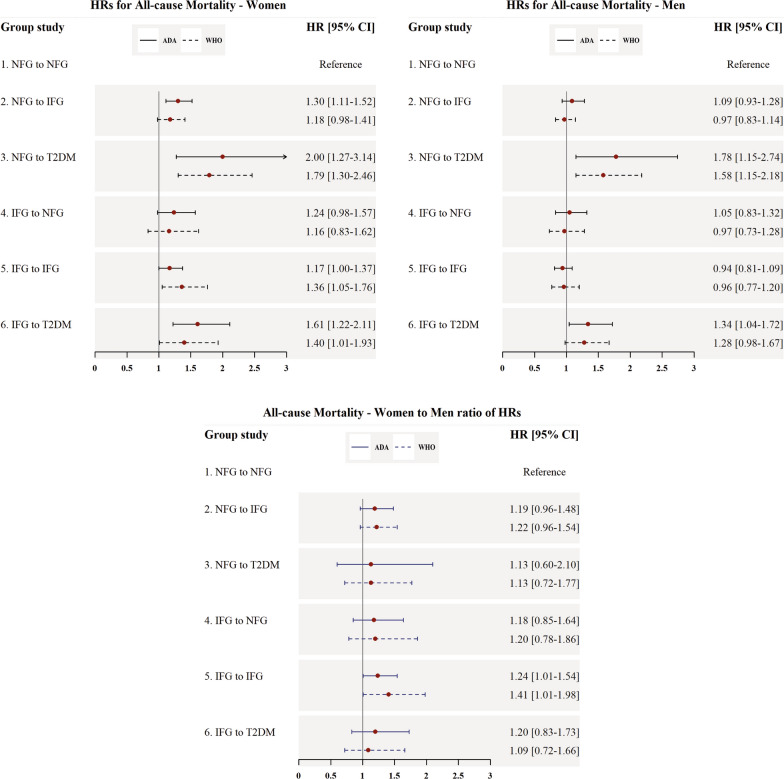
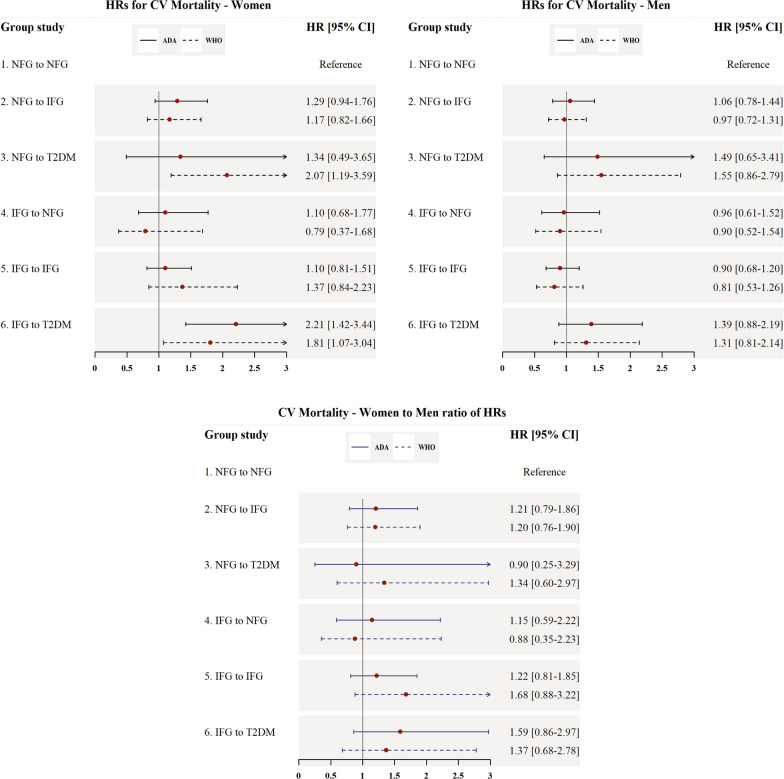
During follow-up, 2,362 all-cause mortality events were recorded. Among women, all categories of FPG change, excluding IFG-NFG (HR, 95%CI 1.24 (0.98-1.57), p = 0.07), were associated with a higher risk of all-cause mortality compared to the NFG-NFG category. Moreover, women in IFG-T2DM group were at increased risk for CV mortality (2.21 (1.42-3.44)). We also found that women in NFG-IFG (1.52 (1.20-1.91)), NFG-T2DM (2.90 (1.52-5.51)), and IFG-IFG (1.30 (1.02-1.66)) categories had a higher risk for cancer mortality. However, among men, a higher risk of all-cause mortality was found for only two groups of NFG-T2DM (1.78 (1.15-2.74)) and IFG-T2DM (1.34 (1.04-1.72)). Women with IFG-IFG had a 24% higher risk for all-cause mortality events than their men counterparts (RHR; 1.24 (1.01-1.54)). After further adjustment for physical activity, results were in line with the main findings, excluding T2DM up to six years after the measurement period and early mortality events.
In women, the IFG status, whether as incident, persistent, or converted to T2DM, had a higher risk for mortality events; however, among men, only conversion to T2DM conferred an excess risk of all-cause mortality.
我们旨在评估在 18 年的随访期间,3 年内空腹血糖(FPG)状态变化对无 2 型糖尿病(T2DM)个体全因、心血管(CV)和癌症死亡风险的性别特异性影响。
研究人群包括来自三个基于人群的队列研究的 14378 名年龄在 30-60 岁(8272 名女性)的参与者,这些研究包括社区动脉粥样硬化风险研究、多民族动脉粥样硬化研究和德黑兰血脂和血糖研究。根据 FPG 状态约三年的变化,将受试者分为六类:(1)正常 FPG(NFG)至 NFG(参考类别);(2)NFG 至空腹血糖受损(IFG)(即 126> FPG≥100mg/dl);(3)NFG 至 T2DM;(4)IFG 至 NFG;(5)IFG 至 IFG;(6)IFG 至 T2DM。使用多变量分层 Cox 回归,调整年龄、体重指数(BMI)、BMI 变化、吸烟状况、高血压和高胆固醇血症,以估计全因和特定原因死亡率事件的危险比(HR(95%CI))。还估计了每个类别中女性与男性的 HR 比值(RHR)。
在随访期间,记录了 2362 例全因死亡事件。在女性中,与 NFG-NFG 类别相比,除 IFG-NFG(HR,95%CI 1.24(0.98-1.57),p=0.07)外,所有 FPG 变化类别均与全因死亡风险增加相关。此外,IFG-T2DM 组的女性发生 CV 死亡率的风险增加(2.21(1.42-3.44))。我们还发现,女性 NFG-IFG(1.52(1.20-1.91))、NFG-T2DM(2.90(1.52-5.51))和 IFG-IFG(1.30(1.02-1.66))组的癌症死亡率风险更高。然而,在男性中,只有 NFG-T2DM(1.78(1.15-2.74))和 IFG-T2DM(1.34(1.04-1.72))两个组的全因死亡率风险更高。IFG-IFG 的女性全因死亡率事件的风险比其男性对应者高 24%(RHR;1.24(1.01-1.54))。在进一步调整体力活动后,结果与主要发现一致,排除了 T2DM 在测量期后六年及早期死亡事件。
在女性中,IFG 状态,无论是新发、持续还是转化为 T2DM,都会增加死亡事件的风险;然而,在男性中,只有转化为 T2DM 会增加全因死亡的风险。