Center of Innovation in Long-Term Services and Supports, Veterans Administration Medical Center, Providence, Rhode Island.
Department of Health Services, Policy and Practice, School of Public Health, Brown University, Providence, Rhode Island.
JAMA Netw Open. 2022 Dec 1;5(12):e2245417. doi: 10.1001/jamanetworkopen.2022.45417.
A SARS-CoV-2 vaccine booster dose has been recommended for all nursing home residents. However, data on the effectiveness of an mRNA vaccine booster in preventing infection, hospitalization, and death in this vulnerable population are lacking.
To evaluate the association between receipt of a SARS-CoV-2 mRNA vaccine booster and prevention of infection, hospitalization, or death among nursing home residents.
DESIGN, SETTING, AND PARTICIPANTS: This cohort study emulated sequentially nested target trials for vaccination using data from 2 large multistate US nursing home systems: Genesis HealthCare, a community nursing home operator (system 1) and Veterans Health Administration community living centers (VHA CLCs; system 2). The cohort included long-term (≥100 days) nursing home residents (10 949 residents from 202 community nursing homes and 4321 residents from 128 VHA CLCs) who completed a 2-dose series of an mRNA vaccine (either BNT162b2 [Pfizer-BioNTech] or mRNA-1273 [Moderna]) and were eligible for a booster dose between September 22 and November 30, 2021. Residents were followed up until March 8, 2022.
Receipt of a third mRNA vaccine dose, defined as a booster dose (boosted group), or nonreceipt of a booster dose (unboosted group) on an eligible target trial date. If participants in the unboosted group received a booster dose on a later target trial date, they were included in the booster group for that target trial; thus, participants could be included in both the boosted and unboosted groups.
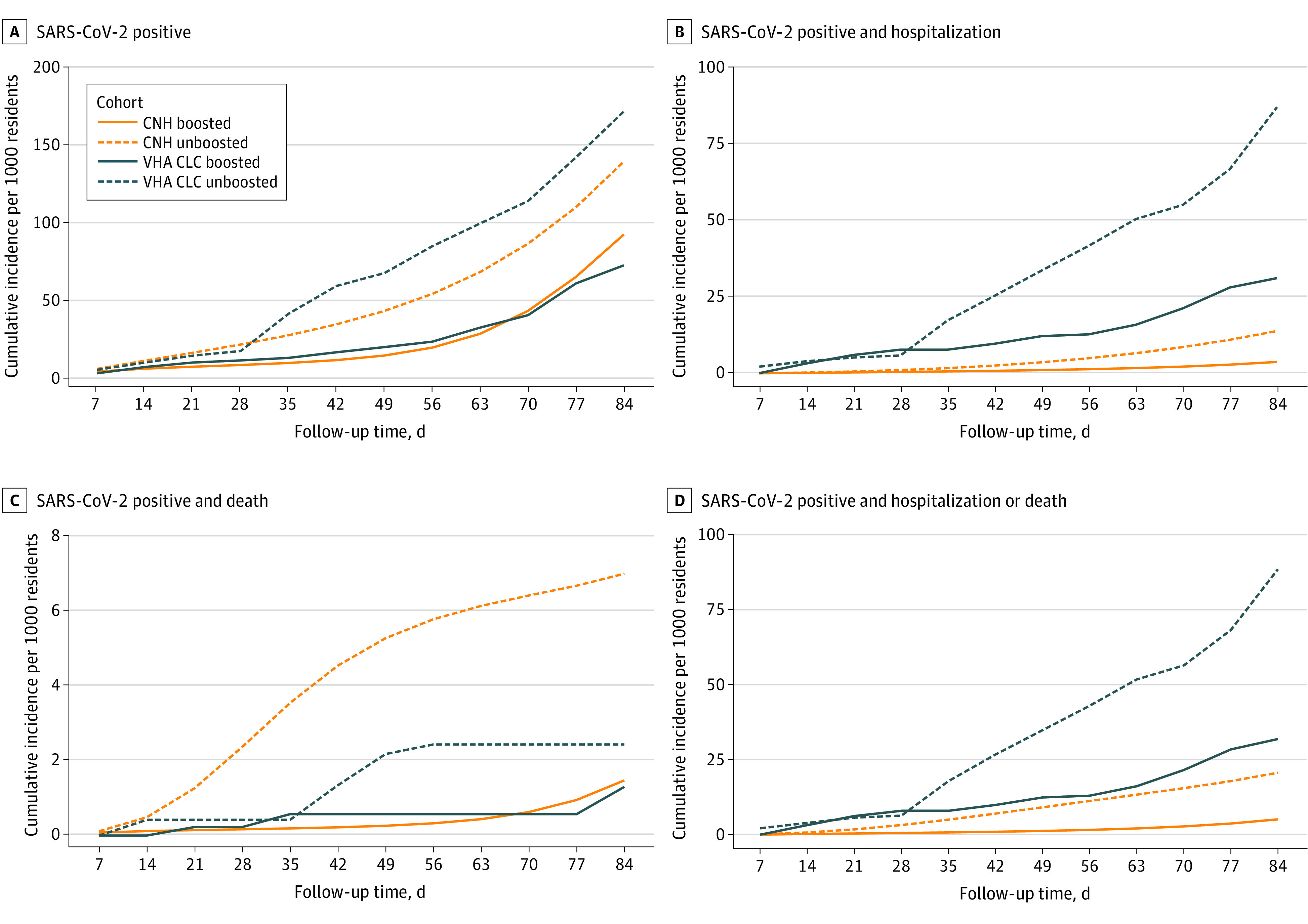
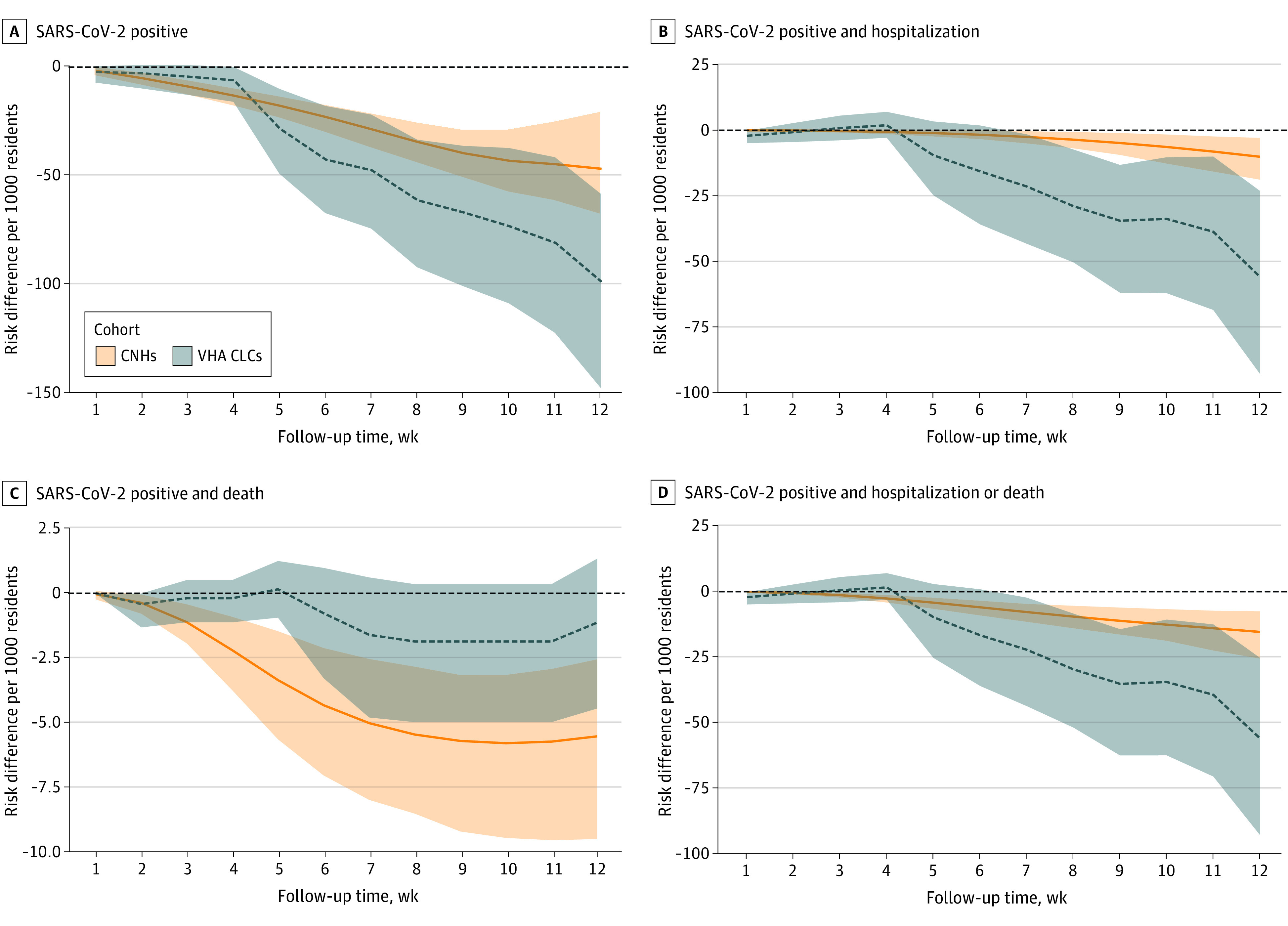
Test-confirmed SARS-CoV-2 infection, hospitalization, or death was followed up to 12 weeks after booster vaccination. The primary measure of estimated vaccine effectiveness was the ratio of cumulative incidences in the boosted group vs the unboosted group at week 12, adjusted with inverse probability weights for treatment and censoring.
System 1 included 202 community nursing homes; among 8332 boosted residents (5325 [63.9%] female; 6685 [80.2%] White) vs 10 886 unboosted residents (6865 [63.1%] female; 8651 [79.5%] White), the median age was 78 (IQR, 68-87) years vs 78 (IQR, 68-86) years. System 2 included 128 VHA CLCs; among 3289 boosted residents (3157 [96.0%] male; 1950 [59.3%] White) vs 4317 unboosted residents (4151 [96.2%] male; 2434 [56.4%] White), the median age was 74 (IQR, 70-80) vs 74 (IQR, 69-80) years. Booster vaccination was associated with reductions in SARS-CoV-2 infections of 37.7% (95% CI, 25.4%-44.2%) in system 1 and 57.7% (95% CI, 43.5%-67.8%) in system 2. For hospitalization, reductions of 74.4% (95% CI, 44.6%-86.2%) in system 1 and 64.1% (95% CI, 41.3%-76.0%) in system 2 were observed. Estimated vaccine effectiveness for death associated with SARS-CoV-2 was 87.9% (95% CI, 75.9%-93.9%) in system 1; however, although a reduction in death was observed in system 2 (46.6%; 95% CI, -34.6% to 94.8%), this reduction was not statistically significant. A total of 45 SARS-CoV-2-associated deaths occurred in system 1 and 18 deaths occurred in system 2. For the combined end point of SARS-CoV-2-associated hospitalization or death, boosted residents in system 1 had an 80.3% (95% CI, 65.7%-88.5%) reduction, and boosted residents in system 2 had a 63.8% (95% CI, 41.4%-76.1%) reduction.
In this study, during a period in which both the Delta and Omicron variants were circulating, SARS-CoV-2 booster vaccination was associated with significant reductions in SARS-CoV-2 infections, hospitalizations, and the combined end point of hospitalization or death among residents of 2 US nursing home systems. These findings suggest that administration of vaccine boosters to nursing home residents may have an important role in preventing COVID-19-associated morbidity and mortality.
建议所有养老院居民接种 SARS-CoV-2 疫苗加强针。然而,关于这种脆弱人群中 mRNA 疫苗加强针在预防感染、住院和死亡方面的有效性的数据尚缺乏。
评估养老院居民接种 SARS-CoV-2 mRNA 疫苗加强针与预防感染、住院或死亡的相关性。
设计、地点和参与者:本队列研究使用来自美国两个大型多州养老院系统的数据模拟了连续嵌套的疫苗接种目标试验:Genesis HealthCare(社区养老院运营商)和退伍军人事务部社区生活中心(VHA CLC;系统 2)。该队列包括在社区养老院(202 家)和 VHA CLC(128 家)居住 100 天以上的长期(≥100 天)养老院居民(10949 名居民和 4321 名居民),他们完成了 2 剂 mRNA 疫苗(BNT162b2[辉瑞-BioNTech]或 mRNA-1273[Moderna])接种,并符合加强针接种条件,接种时间在 2021 年 9 月 22 日至 11 月 30 日之间。居民随访至 2022 年 3 月 8 日。
接种第三剂 mRNA 疫苗,定义为加强针(加强组)或未接种加强针(未加强组),接种日期符合目标试验条件。如果未加强组的参与者在后续目标试验日接种了加强针,则将其纳入该目标试验的加强组;因此,参与者可能同时被纳入加强组和未加强组。
在加强针接种后 12 周内,跟踪检测到的 SARS-CoV-2 感染、住院或死亡。估计疫苗有效性的主要衡量指标是加强组与未加强组在第 12 周的累积发病率之比,通过对治疗和删失进行逆概率加权进行调整。
系统 1 包括 202 家社区养老院;在 8332 名加强组居民(5325 名女性[63.9%];6685 名白人[80.2%])与 10886 名未加强组居民(6865 名女性[63.1%];8651 名白人[79.5%])中,中位年龄为 78(IQR,68-87)岁和 78(IQR,68-86)岁。系统 2 包括 128 家 VHA CLC;在 3289 名加强组居民(3157 名男性[96.0%];1950 名白人[59.3%])与 4317 名未加强组居民(4151 名男性[96.2%];2434 名白人[56.4%])中,中位年龄为 74(IQR,70-80)岁和 74(IQR,69-80)岁。加强针接种与 SARS-CoV-2 感染减少相关,系统 1 中减少了 37.7%(95%CI,25.4%-44.2%),系统 2 中减少了 57.7%(95%CI,43.5%-67.8%)。对于住院,系统 1 中减少了 74.4%(95%CI,44.6%-86.2%),系统 2 中减少了 64.1%(95%CI,41.3%-76.0%)。与 SARS-CoV-2 相关的死亡的估计疫苗有效性在系统 1 中为 87.9%(95%CI,75.9%-93.9%);然而,尽管系统 2 中观察到死亡减少(46.6%;95%CI,-34.6%至 94.8%),但这一减少没有统计学意义。系统 1 中发生了 45 例与 SARS-CoV-2 相关的死亡,系统 2 中发生了 18 例死亡。对于 SARS-CoV-2 相关住院或死亡的综合终点,系统 1 中加强组居民的住院或死亡减少了 80.3%(95%CI,65.7%-88.5%),系统 2 中加强组居民的住院或死亡减少了 63.8%(95%CI,41.4%-76.1%)。
在这项研究中,在 Delta 和 Omicron 变异株流行期间,SARS-CoV-2 加强针接种与美国两个养老院系统中居民 SARS-CoV-2 感染、住院和住院或死亡综合终点的显著减少相关。这些发现表明,为养老院居民接种疫苗加强针可能在预防 COVID-19 相关发病率和死亡率方面发挥重要作用。