Baritussio Anna, Cheng Chun-Yan, Lorenzoni Giulia, Basso Cristina, Rizzo Stefania, De Gaspari Monica, Fachin Francesco, Giordani Andrea Silvio, Ocagli Honoria, Pontara Elena, Cattini Maria Grazia Peloso, Bison Elisa, Gallo Nicoletta, Plebani Mario, Tarantini Giuseppe, Iliceto Sabino, Gregori Dario, Marcolongo Renzo, Caforio Alida Linda Patrizia
Cardiology, Department of Cardiac, Thoracic, Vascular Sciences and Public Health, University of Padua, 35128 Padua, Italy.
Statistics, Department of Cardiac, Thoracic, Vascular Sciences and Public Health, University of Padua, 35128 Padua, Italy.
J Clin Med. 2022 Nov 29;11(23):7068. doi: 10.3390/jcm11237068.
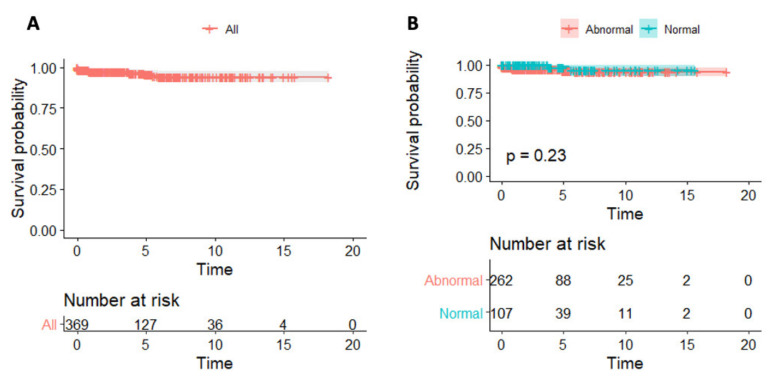
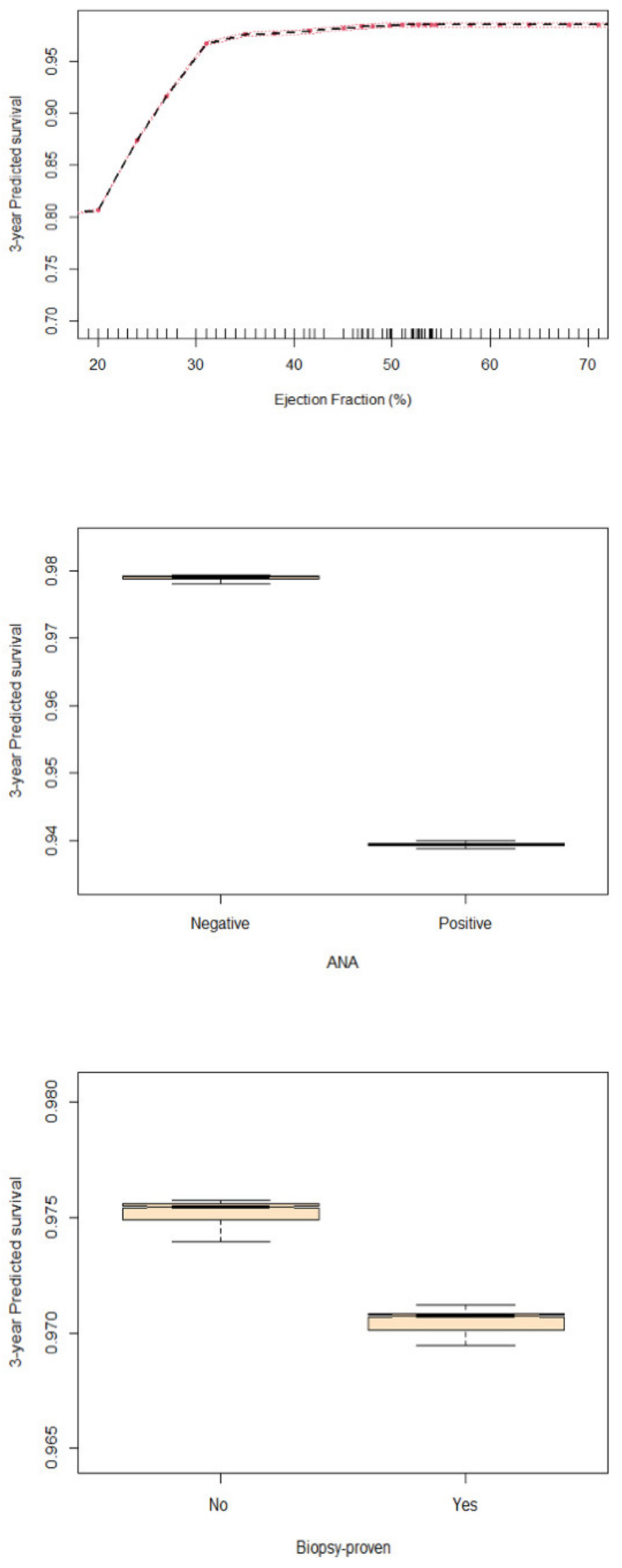
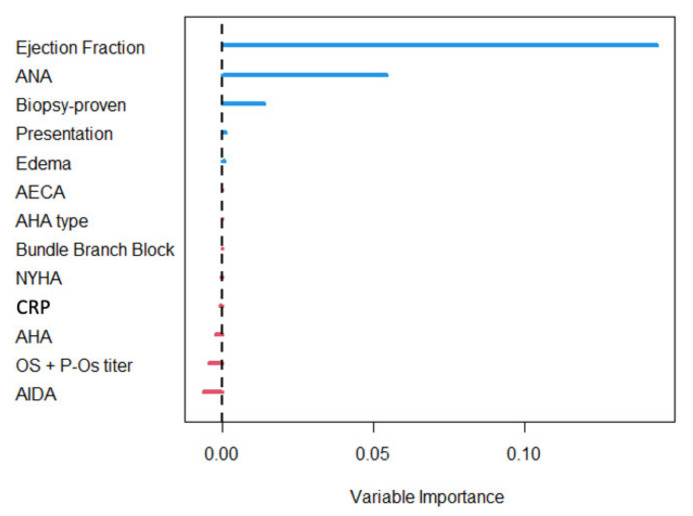
Aims: The role of inflammation markers in myocarditis is unclear. We assessed the diagnostic and prognostic correlates of C-reactive protein (CRP) at diagnosis in patients with myocarditis. Methods and results: We retrospectively enrolled patients with clinically suspected (CS) or biopsy-proven (BP) myocarditis, with available CRP at diagnosis. Clinical, laboratory and imaging data were collected at diagnosis and at follow-up visits. To evaluate predictors of death/heart transplant (Htx), a machine-learning approach based on random forest for survival data was employed. We included 409 patients (74% males, aged 37 ± 15, median follow-up 2.9 years). Abnormal CRP was reported in 288 patients, mainly with CS myocarditis (p < 0.001), recent viral infection, shorter symptoms duration (p = 0.001), chest pain (p < 0.001), better functional class at diagnosis (p = 0.018) and higher troponin I values (p < 0.001). Death/Htx was reported in 13 patients, of whom 10 had BP myocarditis (overall 10-year survival 94%). Survival rates did not differ according to CRP levels (p = 0.23). The strongest survival predictor was LVEF, followed by anti-nuclear auto-antibodies (ANA) and BP status. Conclusions: Raised CRP at diagnosis identifies patients with CS myocarditis and less severe clinical features, but does not contribute to predicting survival. Main death/Htx predictors are reduced LVEF, BP diagnosis and positive ANA.
炎症标志物在心肌炎中的作用尚不清楚。我们评估了心肌炎患者诊断时C反应蛋白(CRP)的诊断及预后相关性。
我们回顾性纳入了临床疑似(CS)或经活检证实(BP)的心肌炎患者,这些患者诊断时可获得CRP数据。在诊断时及随访时收集临床、实验室及影像学数据。为评估死亡/心脏移植(Htx)的预测因素,采用了基于随机森林的生存数据机器学习方法。我们纳入了409例患者(74%为男性,年龄37±15岁,中位随访时间2.9年)。288例患者CRP异常,主要为CS心肌炎患者(p<0.001),伴有近期病毒感染、症状持续时间较短(p=0.001)、胸痛(p<0.001)、诊断时心功能分级较好(p=0.018)及肌钙蛋白I值较高(p<0.001)。13例患者发生死亡/Htx,其中10例为BP心肌炎患者(总体10年生存率94%)。生存率根据CRP水平无差异(p=0.23)。最强的生存预测因素是左室射血分数(LVEF),其次是抗核自身抗体(ANA)及BP状态。
诊断时CRP升高可识别CS心肌炎患者及临床特征较轻者,但无助于预测生存。主要的死亡/Htx预测因素是LVEF降低、BP诊断及ANA阳性。