Department of Pharmacy, West China Second University Hospital, Sichuan University, Chengdu, China.
Evidence-Based Pharmacy Center, West China Second University Hospital, Sichuan University, Chengdu, 610041, China.
BMC Anesthesiol. 2022 Dec 22;22(1):399. doi: 10.1186/s12871-022-01892-2.
Intranasal midazolam and ketamine have been widely used as sedative premedication in children. It is difficult to determine which one yields better sedative effects for clinical practice. We conducted the present meta-analysis by summarizing the evidences to evaluate the efficacy and safety of intranasal midazolam versus intranasal ketamine as sedative premedication in pediatric patients.
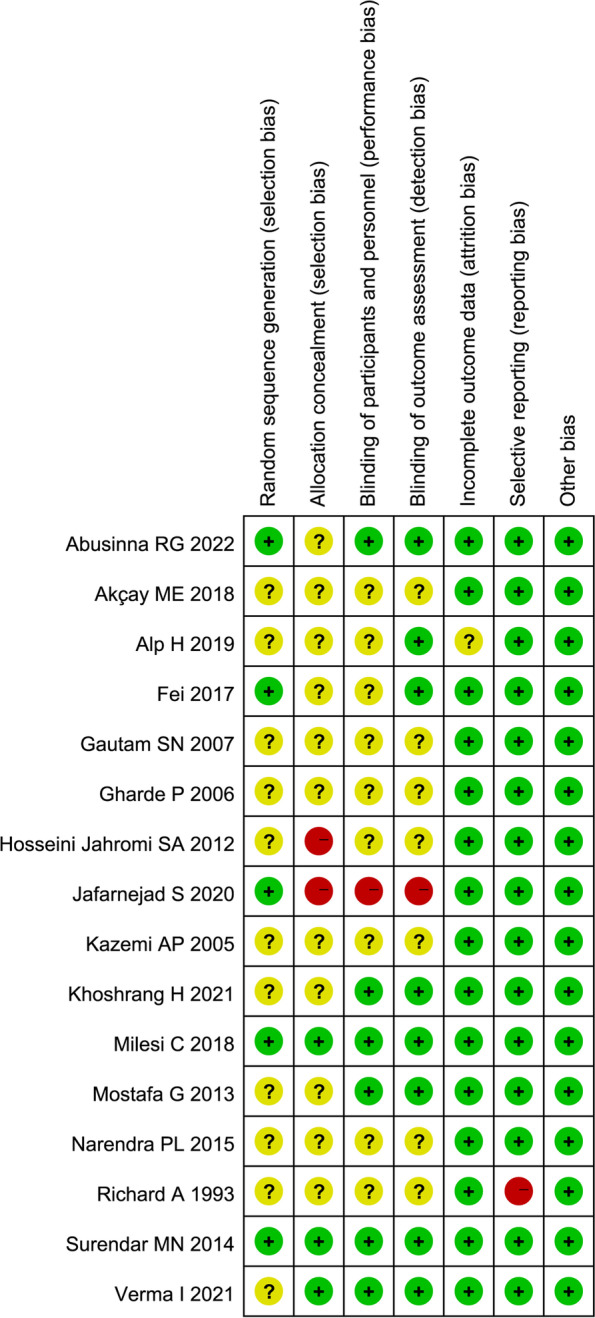
We searched PubMed, Embase, and Cochrane Library from inception to April 2022. All randomized controlled trials (RCTs) used intranasal midazolam and ketamine as sedatives in children were enrolled. The risk of bias in RCTs was assessed by Cochrane risk of bias tool. Condition of parental separation, anesthesia induction or facemask acceptance, sedation level, different hemodynamic parameters and adverse events were considered as the outcomes in our study.
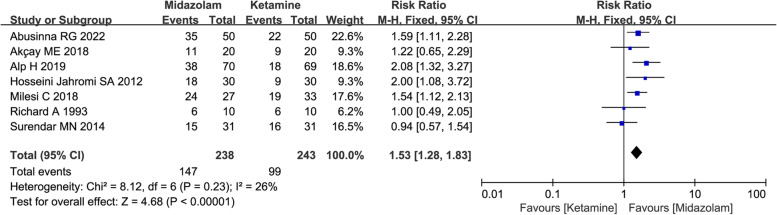
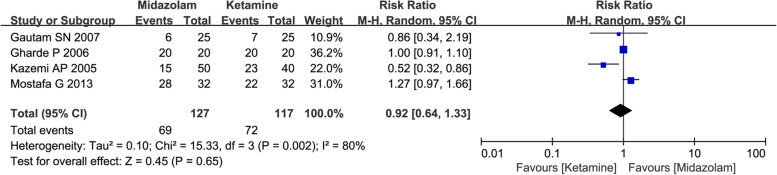
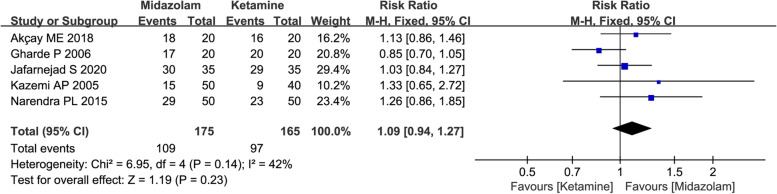
A total of 16 studies with 1066 patients were enrolled. Compared with midazolam, administration of intranasal ketamine might be associated with severer changes in hemodynamics parameters including mean blood pressure (SMD = -0.53, with 95% CI [-0.93, -0.13]) and heart rate (HR) (SMD = -1.39, with 95% CI [-2.84, 0.06]). Meanwhile, administration of intranasal midazolam was associated with more satisfactory sedation level (61.76% vs 40.74%, RR = 1.53, with 95%CI [1.28, 1.83]), more rapid onset of sedation (SMD = -0.59, with 95%CI [-0.90, -0.28]) and more rapid recovery (SMD = -1.06, with 95%CI [-1.83, -0.28]). Current evidences also indicated that the differences of various adverse effects between two groups were not significant.
Given that administration of midazolam via intranasal route provides more satisfactory sedative level with less fluctuation of hemodynamics parameters and more rapid onset and recovery, it might be considered as the preferred sedative premedication for pediatric patients compared to ketamine. However, the widespread evidences with low or moderate quality indicated that superiority of intranasal midazolam in pediatric sedation needs to be confirmed by more studies with high quality and large sample size in future.
The protocol of present study was registered with PROSPERO (CRD42022321348).
鼻内咪达唑仑和氯胺酮已广泛用于儿童镇静前用药。很难确定哪种药物在临床实践中具有更好的镇静效果。我们通过总结证据进行了这项荟萃分析,以评估鼻内咪达唑仑与鼻内氯胺酮作为儿科患者镇静前用药的疗效和安全性。
我们从建库到 2022 年 4 月在 PubMed、Embase 和 Cochrane 图书馆进行了检索。所有使用鼻内咪达唑仑和氯胺酮作为儿童镇静剂的随机对照试验(RCT)均被纳入。通过 Cochrane 偏倚风险工具评估 RCT 的偏倚风险。父母分离、麻醉诱导或面罩接受情况、镇静程度、不同的血液动力学参数和不良事件被视为我们研究的结果。
共纳入 16 项研究,共 1066 名患者。与咪达唑仑相比,鼻内给予氯胺酮可能与更严重的血液动力学参数变化相关,包括平均血压(SMD=-0.53,95%CI[-0.93,-0.13])和心率(HR)(SMD=-1.39,95%CI[-2.84,0.06])。同时,鼻内给予咪达唑仑与更满意的镇静水平相关(61.76% vs 40.74%,RR=1.53,95%CI[1.28,1.83]),镇静起效更快(SMD=-0.59,95%CI[-0.90,-0.28])和更快恢复(SMD=-1.06,95%CI[-1.83,-0.28])。目前的证据还表明,两组之间各种不良反应的差异不显著。
鉴于鼻内给予咪达唑仑可提供更满意的镇静水平,血液动力学参数波动较小,起效和恢复更快,与氯胺酮相比,鼻内给予咪达唑仑可能被认为是儿科患者首选的镇静前用药。然而,目前证据质量较低或中等,表明鼻内咪达唑仑在儿科镇静中的优势需要更多高质量、大样本量的研究来进一步证实。
本研究方案已在 PROSPERO(CRD42022321348)注册。