Ademuyiwa Foluso O, Gao Feng, Street Cherease R, Chen Ina, Northfelt Donald W, Wesolowski Robert, Arora Mili, Brufsky Adam, Dees E Claire, Santa-Maria Cesar A, Connolly Roisin M, Force Jeremy, Moreno-Aspitia Alvaro, Herndon John M, Carmody Madelyn, Davies Sherri R, Larson Sarah, Pfaff Kathleen L, Jones Stephanie M, Weirather Jason L, Giobbie-Hurder Anita, Rodig Scott J, Liu Zheng, Hagemann Ian S, Sharon Elad, Gillanders William E
Washington University School of Medicine, St Louis, MO, 63110, USA.
Mayo Clinic, Phoenix, AZ, 85054, USA.
NPJ Breast Cancer. 2022 Dec 30;8(1):134. doi: 10.1038/s41523-022-00500-3.
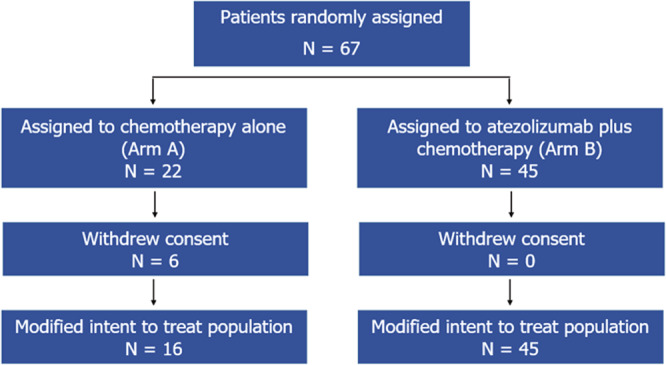
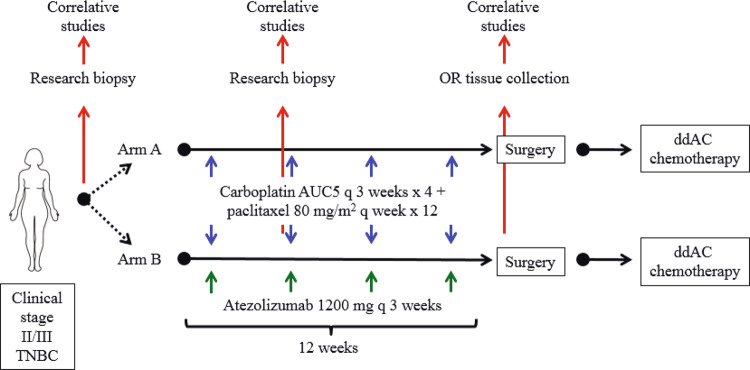
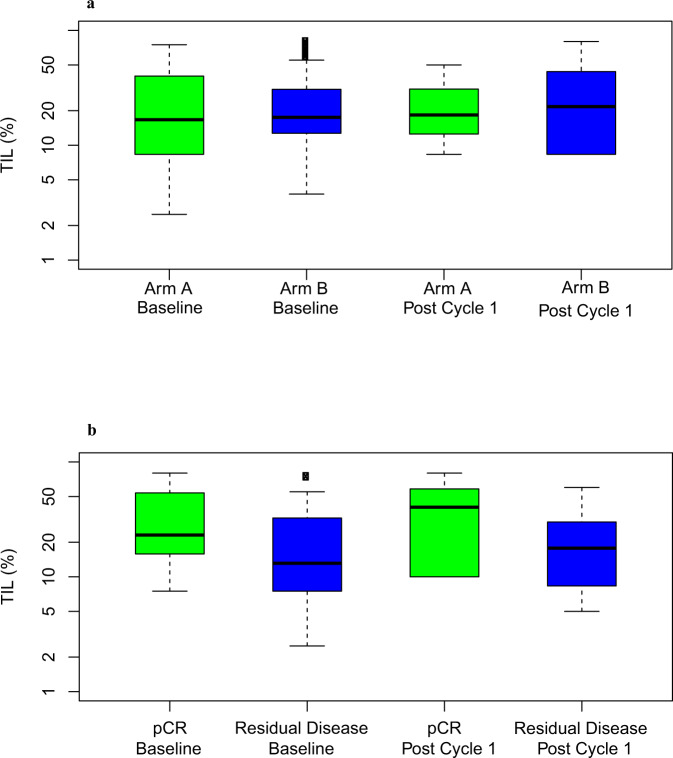
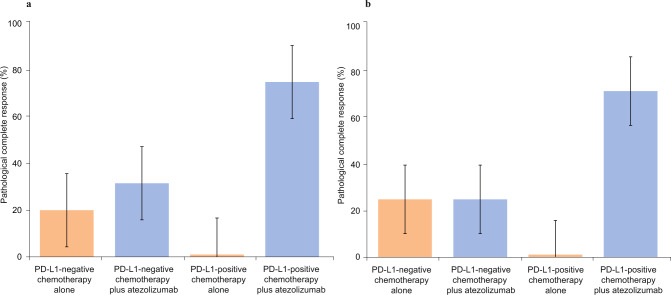
Atezolizumab with chemotherapy has shown improved progression-free and overall survival in patients with metastatic PD-L1 positive triple negative breast cancer (TNBC). Atezolizumab with anthracycline- and taxane-based neoadjuvant chemotherapy has also shown increased pathological complete response (pCR) rates in early TNBC. This trial evaluated neoadjuvant carboplatin and paclitaxel with or without atezolizumab in patients with clinical stages II-III TNBC. The co-primary objectives were to evaluate if chemotherapy and atezolizumab increase pCR rate and tumor infiltrating lymphocyte (TIL) percentage compared to chemotherapy alone in the mITT population. Sixty-seven patients (ages 25-78 years; median, 52 years) were randomly assigned - 22 patients to Arm A, and 45 to Arm B. Median follow up was 6.6 months. In the modified intent to treat population (all patients evaluable for the primary endpoints who received at least one dose of combination therapy), the pCR rate was 18.8% (95% CI 4.0-45.6%) in Arm A, and 55.6% (95% CI 40.0-70.4%) in Arm B (estimated treatment difference: 36.8%, 95% CI 8.5-56.6%; p = 0.018). Grade 3 or higher treatment-related adverse events occurred in 62.5% of patients in Arm A, and 57.8% of patients in Arm B. One patient in Arm B died from recurrent disease during the follow-up period. TIL percentage increased slightly from baseline to cycle 1 in both Arm A (mean ± SD: 0.6% ± 21.0%) and Arm B (5.7% ± 15.8%) (p = 0.36). Patients with pCR had higher median TIL percentages (24.8%) than those with non-pCR (14.2%) (p = 0.02). Although subgroup analyses were limited by the small sample size, PD-L1-positive patients treated with chemotherapy and atezolizumab had a pCR rate of 75% (12/16). The addition of atezolizumab to neoadjuvant carboplatin and paclitaxel resulted in a statistically significant and clinically relevant increased pCR rate in patients with clinical stages II and III TNBC. (Funded by National Cancer Institute).
阿替利珠单抗联合化疗已显示可改善转移性PD-L1阳性三阴性乳腺癌(TNBC)患者的无进展生存期和总生存期。阿替利珠单抗联合基于蒽环类和紫杉烷类的新辅助化疗也显示早期TNBC患者的病理完全缓解(pCR)率有所提高。本试验评估了新辅助卡铂和紫杉醇联合或不联合阿替利珠单抗用于临床II-III期TNBC患者的疗效。共同主要目标是评估在ITT人群中,与单纯化疗相比,化疗联合阿替利珠单抗是否能提高pCR率和肿瘤浸润淋巴细胞(TIL)百分比。67例患者(年龄25-78岁;中位数52岁)被随机分组——22例患者分入A组,45例分入B组。中位随访时间为6.6个月。在改良意向性治疗人群(所有可评估主要终点且接受至少一剂联合治疗的患者)中,A组的pCR率为18.8%(95%CI 4.0-45.6%),B组为55.6%(95%CI 40.0-70.4%)(估计治疗差异:36.8%,95%CI 8.5-56.6%;p = 0.018)。A组62.5%的患者和B组57.8%的患者发生3级或更高等级的治疗相关不良事件。B组有1例患者在随访期间死于疾病复发。A组(均值±标准差:0.6%±21.0%)和B组(5.7%±15.8%)从基线到第1周期TIL百分比均略有增加(p = 0.36)。pCR患者的TIL百分比中位数(24.8%)高于非pCR患者(14.2%)(p = 0.02)。尽管亚组分析因样本量小而受限,但接受化疗联合阿替利珠单抗治疗的PD-L1阳性患者的pCR率为75%(12/16)。在临床II期和III期TNBC患者中,在新辅助卡铂和紫杉醇中添加阿替利珠单抗导致pCR率在统计学上有显著提高且具有临床相关性。(由美国国立癌症研究所资助)