Sonawane Kalyani, Castellano Tara, Washington Christina, Ting Jie, Surinach Andy, Kirshner Carol, Chhatwal Jagpreet, Ayer Turgay, Moore Kathleen
Department of Public Health Sciences, College of Medicine, Medical University of South Carolina, Charleston, SC, USA.
Hollings Cancer Center, Medical University of South Carolina, Charleston, SC, USA.
Gynecol Oncol Rep. 2022 Dec 13;44:101121. doi: 10.1016/j.gore.2022.101121. eCollection 2022 Dec.
Contemporary, real-world data on eligible patients receiving treatment following progression on first-line (1L) recurrent or metastatic cervical cancer (r/mCC) therapy are needed to inform treatment algorithms and identify potential gaps in the r/mCC care continuum.
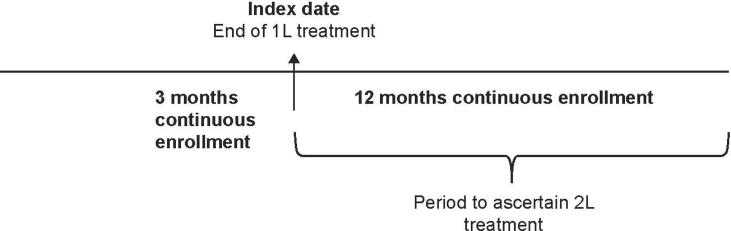
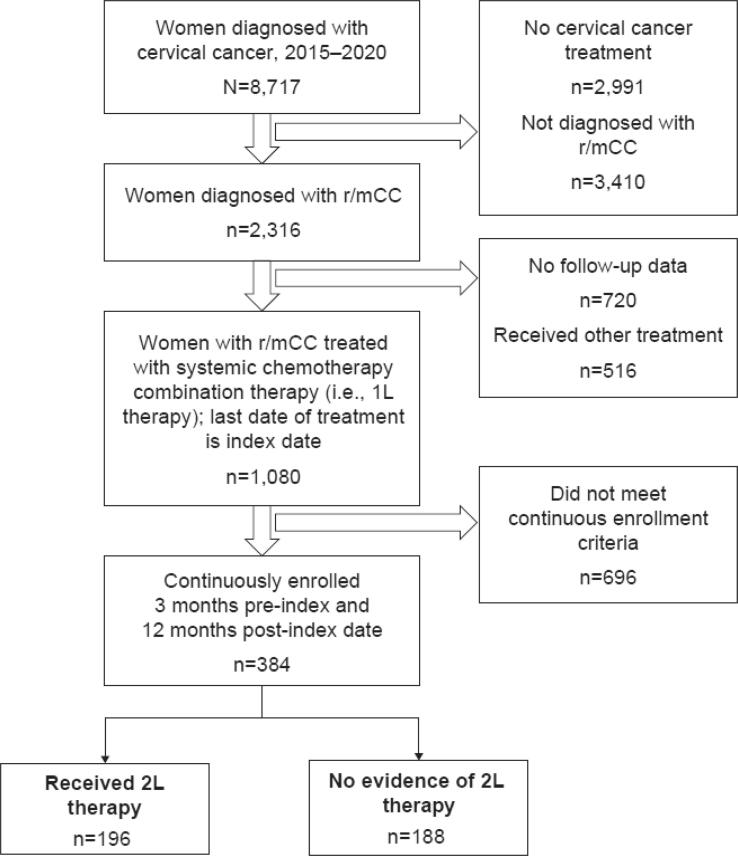
This study estimated the prevalence and predictors of second-line (2L) r/mCC therapy among 1L-treated patients using the 2015-2020 IBM MarketScan® commercial claims database. Women ≥ 18 years diagnosed with cervical cancer and treated with first-line systemic therapies were identified and followed for 12 months from their 1L therapy end date. Women with claims for a new therapy after 60 days but no later than 365 days from the end of 1L treatment were identified as those who progressed and received 2L therapy for r/mCC. Descriptive statistics examined baseline cohort characteristics and multivariable logistic regression model examined the factors associated with receiving 2L treatment.
We identified 384 1L-treated patients with r/mCC with ≥ 12 months of follow-up post-1L treatment. During follow-up, over half (51.0 %) of the 1L-treated r/mCC patients received 2L treatment. Patients from the South and Midwest had a lower likelihood of receiving 2L treatment compared with those living in the Northeast (adjusted odds ratio [aOR] = 0.43; 0.23-0.84) and (aOR = 0.52; 0.28-0.95, respectively). Patients not treated with bevacizumab in 1L were also less likely to receive 2L therapy (aOR = 0.65; 0.43-0.99).
Additional research and targeted outreach efforts are needed to understand geography-, population-, or practice-specific barriers impacting access to 2L therapy among patients with r/mCC.
需要当代真实世界中关于一线(1L)复发或转移性宫颈癌(r/mCC)治疗进展后接受治疗的合格患者的数据,以为治疗算法提供信息并识别r/mCC护理连续过程中的潜在差距。
本研究使用2015 - 2020年IBM MarketScan®商业索赔数据库估计了1L治疗患者中二线(2L)r/mCC治疗的患病率和预测因素。确定年龄≥18岁且诊断为宫颈癌并接受一线全身治疗的女性,并从其1L治疗结束日期开始随访12个月。在1L治疗结束后60天但不迟于365天有新治疗索赔的女性被确定为进展并接受r/mCC的2L治疗的患者。描述性统计检查了基线队列特征,多变量逻辑回归模型检查了与接受2L治疗相关的因素。
我们确定了384例接受1L治疗的r/mCC患者,1L治疗后随访≥12个月。随访期间,超过一半(51.0%)接受1L治疗的r/mCC患者接受了2L治疗。与居住在东北部的患者相比,来自南部和中西部的患者接受2L治疗的可能性较低(调整优势比[aOR]=0.43;0.23 - 0.84)和(aOR = 0.52;0.28 - 0.95,分别)。在1L治疗中未接受贝伐单抗治疗的患者接受2L治疗的可能性也较小(aOR = 0.65;0.43 - 0.99)。
需要进行更多研究和有针对性的推广努力,以了解影响r/mCC患者获得2L治疗的地理、人群或实践特定障碍。