Department of Obstetrics, Gynecology & Reproductive Health, Rutgers New Jersey Medical School, Newark, New Jersey.
Department of Pathology, Johns Hopkins University School of Medicine, Baltimore, Maryland.
Cancer Prev Res (Phila). 2023 Apr 3;16(4):219-227. doi: 10.1158/1940-6207.CAPR-22-0413.
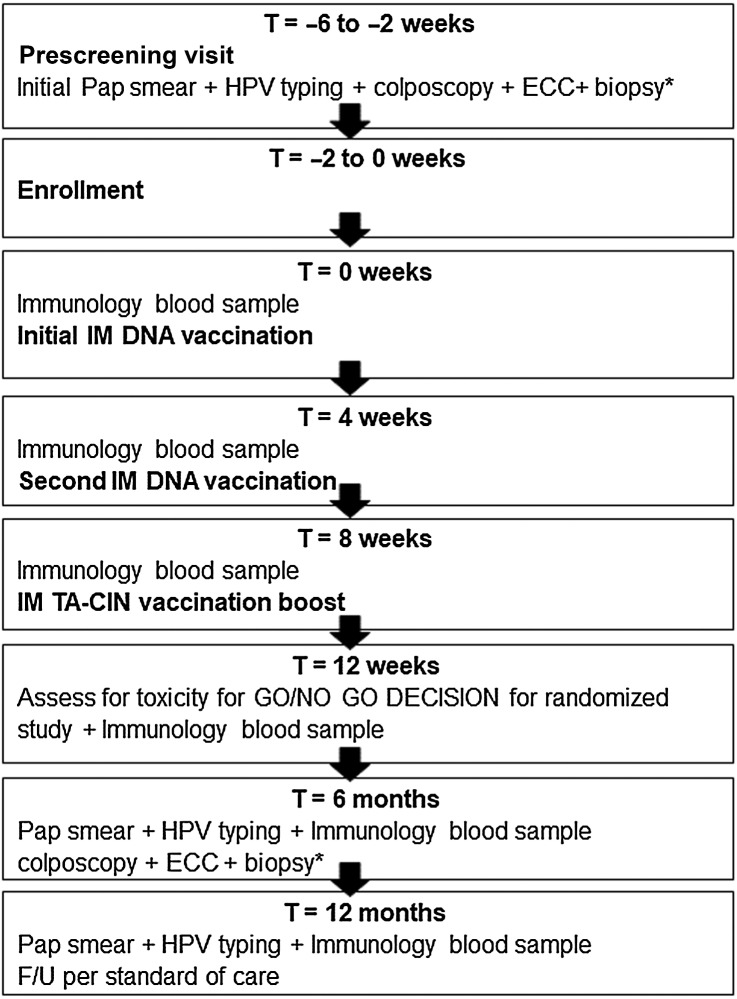
Patients with human papillomavirus type 16 (HPV16) infection and low-grade cervical dysplasia [low-grade squamous intraepithelial lesion (LSIL)/CIN1] or atypical squamous cells [atypical squamous cells of undetermined significance (ASC-US)/atypical squamous cells- cannot exclude high-grade squamous intraepithelial lesion (ASC-H)] require active surveillance for disease progression. A safe and effective immunotherapy to clear HPV16 is an unmet medical need. The safety run-in cohort of a randomized double-blind, placebo-controlled phase II trial of PVX2 [vaccination twice with HPV16-targeting pNGVL4a-Sig/E7(detox)/HSP70 plasmid and once with the HPV16 L2E7E6 fusion protein "TA-CIN"] as immunotherapy for patients with HPV16+ ASC-US, ASC-H, or LSIL/CIN1 (NCT03911076) was recently completed. The primary objective of this cohort was to determine the safety and tolerability of PVX2 vaccination. Subjects were confirmed to have HPV16 infection and LSIL/CIN1, ASC-US, or ASC-H. Adverse events were evaluated using Common Terminology Criteria for Adverse Events v5.0. HPV typing by HPV16 18/45 Aptima Assay was done at baseline, month 6, and month 12, with simultaneous cytology analysis. Cervical biopsies and endocervical curettage were performed at baseline and month 6. In the safety run-in cohort 12 eligible patients were enrolled. Each received three monthly immunizations. One was lost to follow-up after week 12. There were no serious adverse events. A total of five adverse events were noted by 4 patients; 4 were considered not vaccine-related, and one 'unlikely related' by the investigator. At month 6, 45% (5/11) of participants converted to HPV16-negative and 2 others developed CIN2+ and received a loop electrosurgical excision procedure. At month 12, 64% (7/11) were HPV16-negative, including those HPV16-negative at month 6. In conclusion, PVX2 immunotherapy was well tolerated and associated with viral regression, supporting further testing.
This safety run-in study cohort suggests that PVX2 immunotherapy is well tolerated in the target population and is sufficiently safe to warrant further clinical testing in a randomized study. The combined vaccines may facilitate higher-than-expected rate of human papillomavirus type 16 viral clearance 6 and 12 months after treatment, although this requires validation.
目的:评价 HPV16 靶向 pNGVL4a-Sig/E7(detox)/HSP70 质粒和 HPV16 L2E7E6 融合蛋白“TA-CIN”二联免疫接种及三联免疫接种治疗 HPV16 阳性 ASC-US、ASC-H 或 LSIL/CIN1 患者的安全性和免疫原性。
设计:多中心、随机、双盲、安慰剂对照的 II 期临床试验。
地点:在美国和欧洲的 15 个中心。
患者:HPV16 阳性、细胞学 ASC-US、ASC-H 或 LSIL/CIN1。
干预措施:二联免疫接种(n=24):第 0、1 和 6 个月各接种 1 次 pNGVL4a-Sig/E7(detox)/HSP70 质粒和 TA-CIN;三联免疫接种(n=25):第 0、1 和 6 个月各接种 1 次 pNGVL4a-Sig/E7(detox)/HSP70 质粒,第 12 个月接种 TA-CIN。
主要观察指标:主要终点为治疗后 12 个月的安全性和不良事件发生率;次要终点为 HPV16 清除率、抗 HPV16 中和抗体和抗 TA-CIN 抗体滴度。
结果:2 组患者的中位年龄均为 35 岁,均以白人为主,均有 LSIL/CIN1。二联免疫接种组有 1 例患者因不良事件失访,三联免疫接种组有 2 例患者因治疗后 6 个月未发生 HPV16 清除而退出。治疗后 12 个月,二联免疫接种组和三联免疫接种组分别有 88%和 92%的患者 HPV16 清除,差异无统计学意义(P=0.63)。治疗后 6 个月,二联免疫接种组和三联免疫接种组分别有 50%和 56%的患者发生 CIN2+病变,分别有 21%和 16%的患者发生 CIN3+病变。
结论:HPV16 靶向 pNGVL4a-Sig/E7(detox)/HSP70 质粒和 TA-CIN 的二联免疫接种和三联免疫接种治疗 HPV16 阳性 ASC-US、ASC-H 或 LSIL/CIN1 患者是安全的,可诱导 HPV16 清除和 HPV16 特异性免疫应答。