Xue Wenxiu, Shi Jinglong
Department of Thyroid Surgery, The First Affiliated Hospital of Zhengzhou University, Zhenzhou, China.
Department of General Surgery, Guangzhou 12th People's Hospital, Guangzhou, China.
J Gastrointest Oncol. 2022 Dec;13(6):3038-3055. doi: 10.21037/jgo-22-1070.
Mismatch repair-proficient (pMMR) colorectal cancers (CRCs) are thought to be primarily resistant to immune checkpoint inhibitor (ICI) monotherapy. However, recent clinical trials have reported that early-to-mid stage (non-metastatic) CRC responds well to ICI monotherapy. We hypothesized that the efficacy of immunotherapy is linked to a series of gene expression profiles that can characterize the pMMR CRC disease stage.
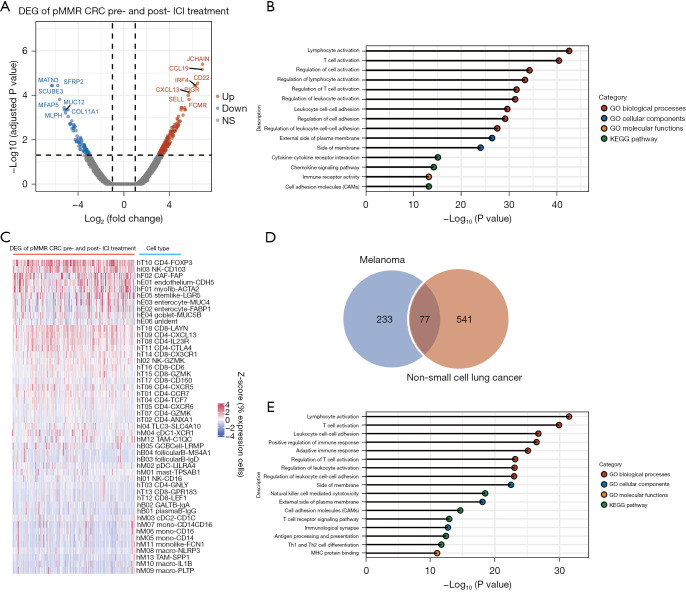
Using The Cancer Genome Atlas (TCGA) CRC data sets, we first investigated transcriptomic features that continuously changed (were continuously upregulated or downregulated) with pMMR CRC disease-stage progression. We defined these gene sets as stage-associated genes. The deconvolution algorithm then enriched these genes with the dynamic changes in the cell type populations of the CRC tumor microenvironment (TME). Finally, the stage-associated genes were cross-referenced to the current transcriptome profile data on ICI treatment of pMMR CRC, which revealed the gene set specifying an effective pMMR tumor response.
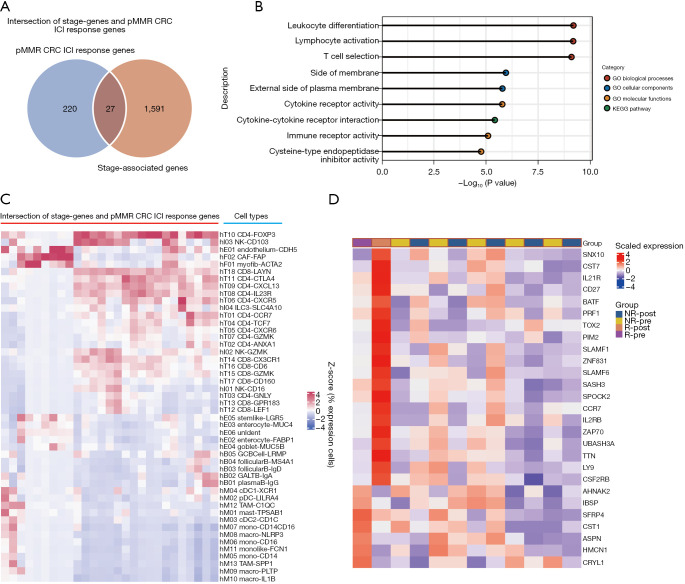
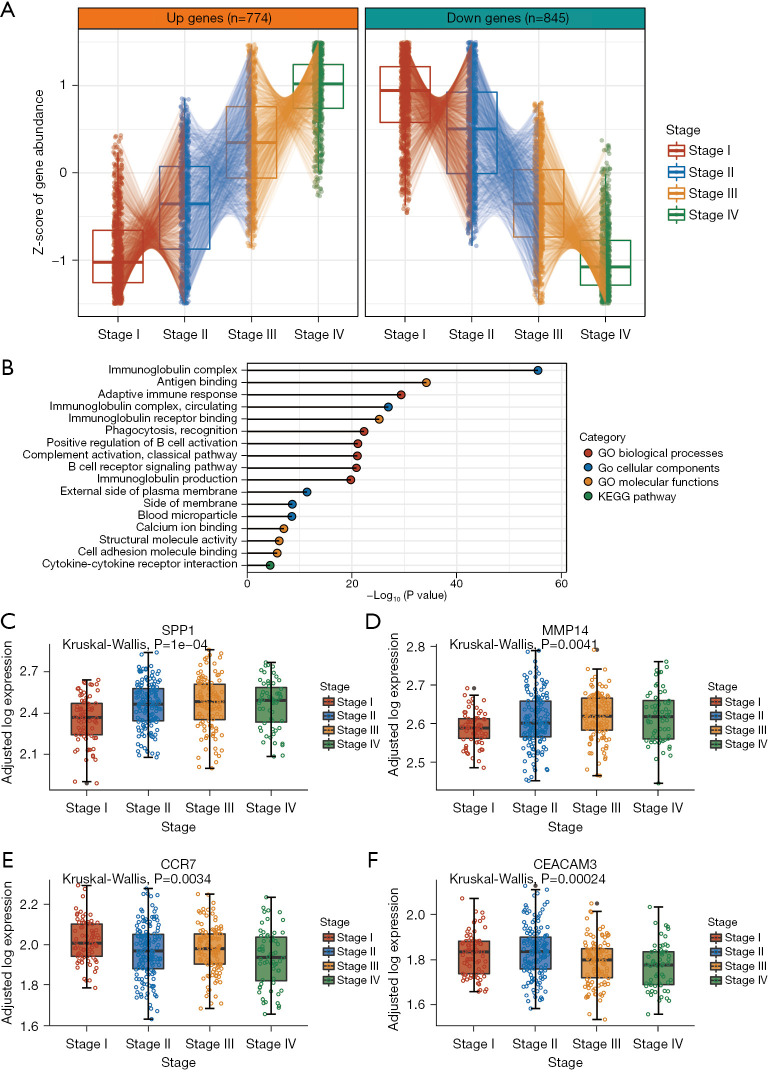
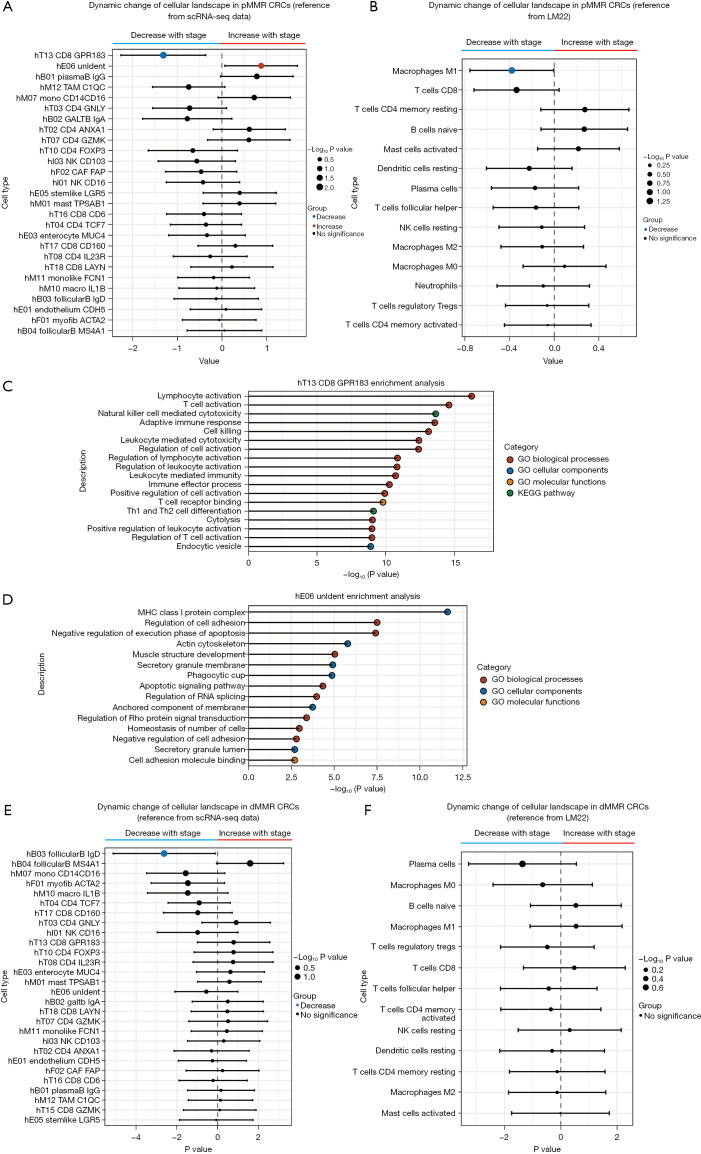
In total, 774 genes were found to increase in expression and 845 genes to decrease in expression as the stage increased. Using deconvolution methods, we discovered 2 major disease stage-associated alterations in the cellular composition of pMMR CRCs, including changes in cell types involved in host immune responses and tumor cell metastasis. The central memory CD8 T cell population decreased as the pMMR CRC disease stage increased, but the endothelial cell populations associated with proliferation and metastasis increased. Using a different cell type annotation set (LM22), we discovered that as the disease progressed, M1 macrophages and CD8 T cells decreased in the TME. In mismatch repair-deficient patients with CRC, however, such a decrease was not observed. Finally, we identified 27 signature genes that can be used to assess ICI efficacy in treatment-naïve patients with pMMR CRC.
The current study sought to identify the underlying molecular mechanisms, pathways, and cell landscapes that explain why early-to-mid stage pMMR CRC responds well to ICI treatment. This analysis might be valuable for the selection of patients who might benefit from immunotherapeutic strategies.
错配修复功能正常(pMMR)的结直肠癌(CRC)被认为对免疫检查点抑制剂(ICI)单药治疗主要耐药。然而,最近的临床试验报告称,早期至中期(非转移性)CRC对ICI单药治疗反应良好。我们假设免疫治疗的疗效与一系列能够表征pMMR CRC疾病阶段的基因表达谱相关。
使用癌症基因组图谱(TCGA)CRC数据集,我们首先研究了随着pMMR CRC疾病阶段进展而持续变化(持续上调或下调)的转录组特征。我们将这些基因集定义为阶段相关基因。然后,反卷积算法利用CRC肿瘤微环境(TME)细胞类型群体的动态变化丰富这些基因。最后,将阶段相关基因与当前关于pMMR CRC的ICI治疗的转录组谱数据进行交叉参考,从而揭示指定有效pMMR肿瘤反应的基因集。
总共发现随着阶段增加,774个基因表达增加,845个基因表达减少。使用反卷积方法,我们在pMMR CRC的细胞组成中发现了2种主要的疾病阶段相关改变,包括宿主免疫反应和肿瘤细胞转移所涉及的细胞类型变化。随着pMMR CRC疾病阶段增加,中央记忆CD8 T细胞群体减少,但与增殖和转移相关的内皮细胞群体增加。使用不同的细胞类型注释集(LM22),我们发现随着疾病进展,TME中的M1巨噬细胞和CD8 T细胞减少。然而,在错配修复缺陷的CRC患者中未观察到这种减少。最后,我们鉴定出27个特征基因,可用于评估初治pMMR CRC患者的ICI疗效。
当前研究旨在确定解释早期至中期pMMR CRC对ICI治疗反应良好的潜在分子机制、途径和细胞格局。该分析对于选择可能从免疫治疗策略中获益的患者可能具有价值。