Association of Dutch Burn Centres, Maasstad Hospital, Rotterdam, the Netherlands.
Trauma Research Unit, Department of Surgery, Erasmus MC, University Medical Center Rotterdam, Rotterdam, the Netherlands.
BMC Geriatr. 2023 Jan 17;23(1):30. doi: 10.1186/s12877-022-03669-1.
The population of elderly patients with burn injuries is growing. Insight into long-term mortality rates of elderly after burn injury and predictors affecting outcome is limited. This study aimed to provide this information.
A multicentre observational retrospective cohort study was conducted in all three Dutch burn centres. Patients aged ≥65 years, admitted with burn injuries between 2009 and 2018, were included. Data were retrieved from electronic patient records and the Dutch Burn Repository R3. Mortality rates and standardized mortality ratios (SMRs) were calculated. Multivariable logistic regression was used to assess predictors for in-hospital mortality and mortality after discharge at 1 year and five-year. Survival analysis was used to assess predictors of five-year mortality.
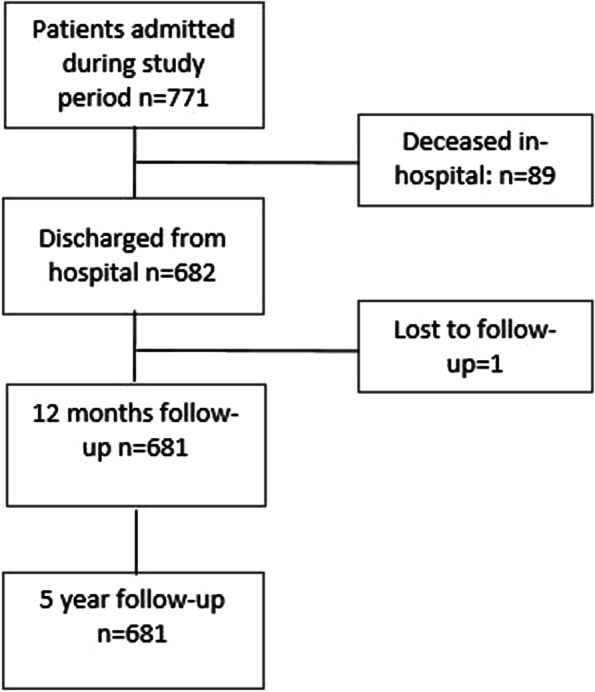
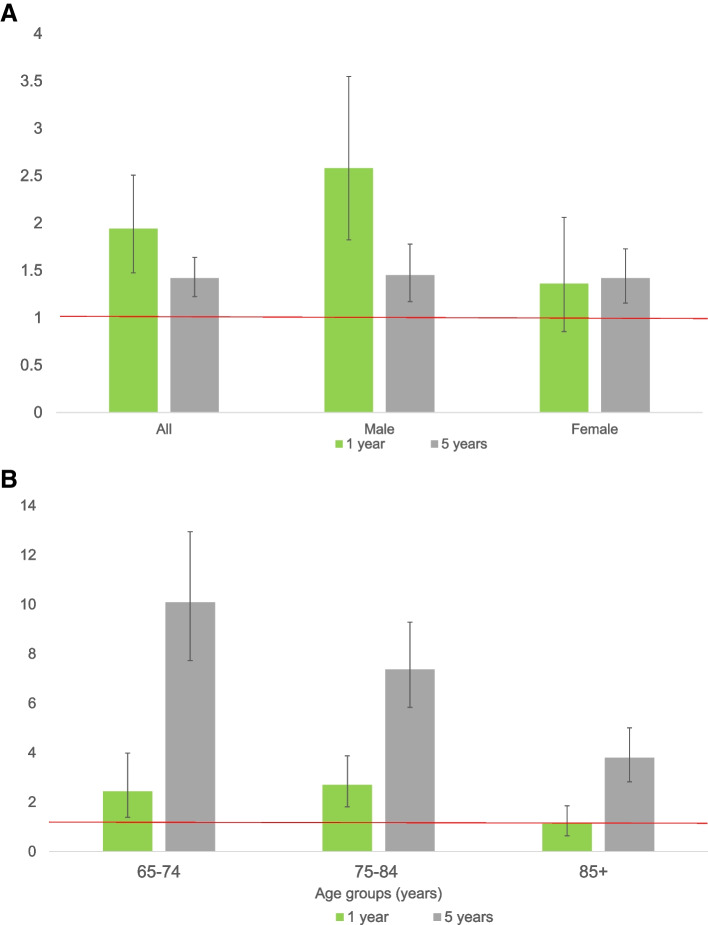
In total, 682/771 admitted patients were discharged. One-year and five-year mortality rates were 8.1 and 23.4%. The SMRs were 1.9(95%CI 1.5-2.5) and 1.4(95%CI 1.2-1.6), respectively. The SMRs were highest in patients aged 75-80 years at 1 year (SMRs 2.7, 95%CI 1.82-3.87) and five-year in patients aged 65-74 years (SMRs 10.1, 95%CI 7.7-13.0). Independent predictors for mortality at 1 year after discharge were higher age (OR 1.1, 95%CI 1.0-1.1), severe comorbidity, (ASA-score ≥ 3) (OR 4.8, 95%CI 2.3-9.7), and a non-home discharge location (OR 2.0, 95%CI 1.1-3.8). The relative risk of dying up to five-year was increased by age (HR 1.1, 95%CI 1.0-1.1), severe comorbidity (HR 2.3, 95%CI 1.6-3.5), and non-home discharge location (HR 2.1, 95%CI 1.4-3.2).
Long-term mortality until five-year after burn injury was higher than the age and sex-matched general Dutch population, and predicted by higher age, severe comorbidity, and a non-home discharge destination. Next to pre-injury characteristics, potential long-lasting systemic consequences on biological mechanisms following burn injuries probably play a role in increased mortality. Decreased health status makes patients more prone to burn injuries, leading to early death.
老年烧伤患者的人数不断增加。对于烧伤后老年患者的长期死亡率以及影响预后的预测因素,我们知之甚少。本研究旨在提供相关信息。
对荷兰三家烧伤中心的所有 65 岁及以上的烧伤患者进行了一项多中心观察性回顾性队列研究。收集患者从电子病历和荷兰烧伤资料库 R3 中提取的数据。计算死亡率和标准化死亡率比(SMR)。采用多变量逻辑回归分析评估院内死亡率以及出院后 1 年和 5 年的死亡率的预测因素。生存分析用于评估 5 年死亡率的预测因素。
共纳入 771 例患者,其中 682 例出院。1 年和 5 年的死亡率分别为 8.1%和 23.4%。SMR 分别为 1.9(95%CI 1.5-2.5)和 1.4(95%CI 1.2-1.6)。75-80 岁患者的 1 年 SMR 最高(SMR 2.7,95%CI 1.82-3.87),65-74 岁患者的 5 年 SMR 最高(SMR 10.1,95%CI 7.7-13.0)。出院后 1 年死亡率的独立预测因素包括年龄较大(OR 1.1,95%CI 1.0-1.1)、严重合并症(ASA 评分≥3)(OR 4.8,95%CI 2.3-9.7)和非家庭出院地点(OR 2.0,95%CI 1.1-3.8)。直至 5 年的死亡相对风险随着年龄(HR 1.1,95%CI 1.0-1.1)、严重合并症(HR 2.3,95%CI 1.6-3.5)和非家庭出院地点(HR 2.1,95%CI 1.4-3.2)的增加而增加。
烧伤后 5 年的长期死亡率高于年龄和性别匹配的荷兰一般人群,且与较高的年龄、严重的合并症和非家庭出院地点有关。除了受伤前的特征外,烧伤后对生物机制的潜在长期系统性影响可能是导致死亡率增加的原因。健康状况的下降使患者更容易受到烧伤的影响,从而导致早期死亡。