Department of Anesthesiology, Critical Care Medicine and Emergency, SS. Annunziata Hospital, Chieti, Italy; Department of Medical, Oral and Biotechnological Sciences, University of Chieti-Pescara, Chieti, Italy.
Pulmonology Unit, Department of Cardiothoracic Surgery, Health Integrated Agency of Friuli Centrale, Udine, Italy.
Pulmonology. 2023 Nov-Dec;29(6):457-468. doi: 10.1016/j.pulmoe.2022.11.002. Epub 2022 Nov 24.
The risk of barotrauma associated with different types of ventilatory support is unclear in COVID-19 patients. The primary aim of this study was to evaluate the effect of the different respiratory support strategies on barotrauma occurrence; we also sought to determine the frequency of barotrauma and the clinical characteristics of the patients who experienced this complication.
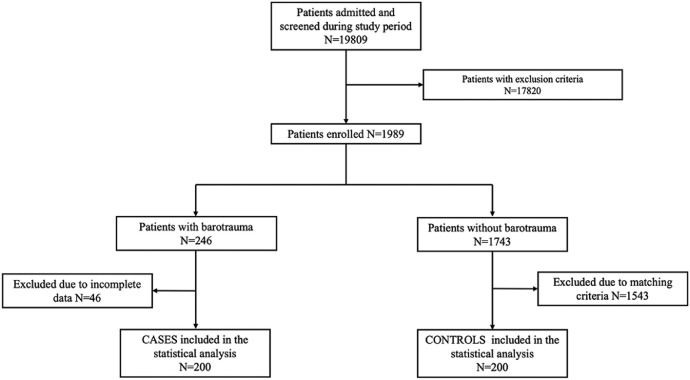
This multicentre retrospective case-control study from 1 March 2020 to 28 February 2021 included COVID-19 patients who experienced barotrauma during hospital stay. They were matched with controls in a 1:1 ratio for the same admission period in the same ward of treatment. Univariable and multivariable logistic regression (OR) were performed to explore which factors were associated with barotrauma and in-hospital death.
We included 200 cases and 200 controls. Invasive mechanical ventilation was used in 39.3% of patients in the barotrauma group, and in 20.1% of controls (p<0.001). Receiving non-invasive ventilation (C-PAP/PSV) instead of conventional oxygen therapy (COT) increased the risk of barotrauma (OR 5.04, 95% CI 2.30 - 11.08, p<0.001), similarly for invasive mechanical ventilation (OR 6.24, 95% CI 2.86-13.60, p<0.001). High Flow Nasal Oxygen (HFNO), compared with COT, did not significantly increase the risk of barotrauma. Barotrauma frequency occurred in 1.00% [95% CI 0.88-1.16] of patients; these were older (p=0.022) and more frequently immunosuppressed (p=0.013). Barotrauma was shown to be an independent risk for death (OR 5.32, 95% CI 2.82-10.03, p<0.001).
C-PAP/PSV compared with COT or HFNO increased the risk of barotrauma; otherwise HFNO did not. Barotrauma was recorded in 1.00% of patients, affecting mainly patients with more severe COVID-19 disease. Barotrauma was independently associated with mortality.
this case-control study was prospectively registered in clinicaltrial.gov as NCT04897152 (on 21 May 2021).
COVID-19 患者使用不同类型通气支持的气压伤风险尚不清楚。本研究的主要目的是评估不同呼吸支持策略对气压伤发生的影响;我们还旨在确定气压伤的发生率以及发生该并发症的患者的临床特征。
这是一项 2020 年 3 月 1 日至 2021 年 2 月 28 日进行的多中心回顾性病例对照研究,纳入了住院期间发生气压伤的 COVID-19 患者。他们与同一病房同一入院期间的对照组以 1:1 的比例进行匹配。采用单变量和多变量逻辑回归(OR)探讨哪些因素与气压伤和院内死亡相关。
我们纳入了 200 例病例和 200 例对照。气压伤组中 39.3%的患者使用有创机械通气,而对照组中为 20.1%(p<0.001)。与常规氧疗(COT)相比,使用无创通气(C-PAP/PSV)增加了气压伤的风险(OR 5.04,95%CI 2.30-11.08,p<0.001),使用有创机械通气(OR 6.24,95%CI 2.86-13.60,p<0.001)也增加了气压伤的风险。与 COT 相比,高流量鼻氧(HFNO)并未显著增加气压伤的风险。气压伤发生率为 1.00%[95%CI 0.88-1.16];这些患者年龄较大(p=0.022),且更常接受免疫抑制治疗(p=0.013)。气压伤是死亡的独立危险因素(OR 5.32,95%CI 2.82-10.03,p<0.001)。
与 COT 或 HFNO 相比,C-PAP/PSV 增加了气压伤的风险;否则 HFNO 没有。气压伤在 1.00%的患者中记录到,主要影响 COVID-19 疾病更严重的患者。气压伤与死亡率独立相关。
这项病例对照研究前瞻性地在 clinicaltrial.gov 上注册为 NCT04897152(2021 年 5 月 21 日)。