Karpin Hana, Vatine Jean-Jacques, Bachar Kirshenboim Yishai, Markezana Aurelia, Weissman-Fogel Irit
Physical Therapy Department, Faculty of Social Welfare and Health Sciences, University of Haifa, Haifa 3498838, Israel.
Reuth Rehabilitation Hospital, Tel Aviv 6772829, Israel.
Biomedicines. 2022 Dec 29;11(1):89. doi: 10.3390/biomedicines11010089.
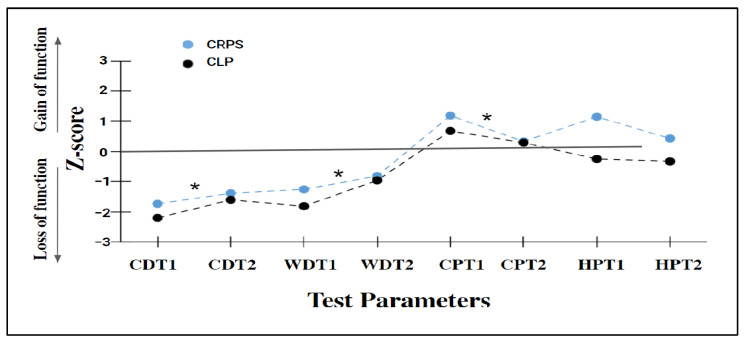
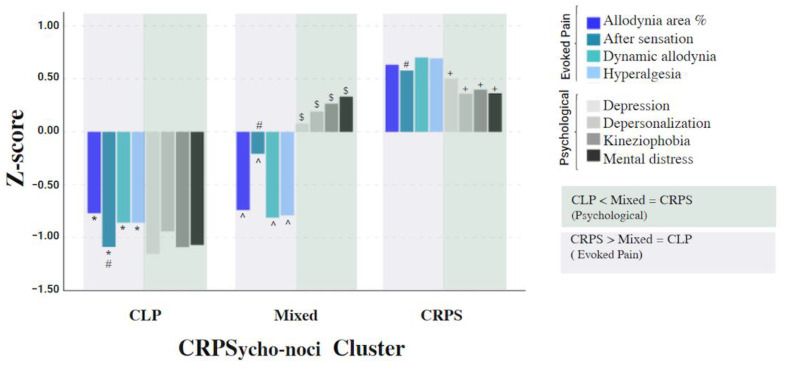
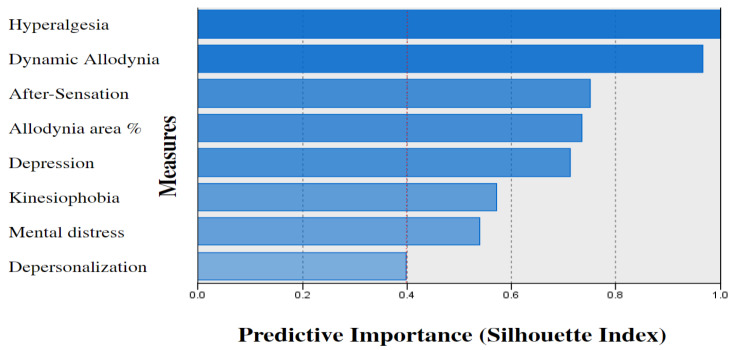
Complex regional pain syndrome (CRPS) taxonomy has been updated with reported subtypes and is defined as primary pain alongside other chronic limb pain (CLP) conditions. We aimed at identifying CRPS clinical phenotypes that distinguish CRPS from other CLP conditions. Cluster analysis was carried out to classify 61 chronic CRPS and 31 CLP patients based on evoked pain (intensity of hyperalgesia and dynamic allodynia, allodynia area, and after-sensation) and psychological (depression, kinesiophobia, mental distress, and depersonalization) measures. Pro-inflammatory cytokine IL-6 and TNF-α serum levels were measured. Three cluster groups were created: ‘CRPS’ (78.7% CRPS; 6.5% CLP); ‘CLP’ (64.5% CLP; 4.9% CRPS), and ‘Mixed’ (16.4% CRPS; 29% CLP). The groups differed in all measures, predominantly in allodynia and hyperalgesia (p < 0.001, η² > 0.58). ‘CRPS’ demonstrated higher psychological and evoked pain measures vs. ‘CLP’. ‘Mixed’ exhibited similarities to ‘CRPS’ in psychological profile and to ‘CLP’ in evoked pain measures. The serum level of TNF-αwas higher in the ‘CRPS’ vs. ‘CLP’ (p < 0.001) groups. In conclusion, pain hypersensitivity reflecting nociplastic pain mechanisms and psychological state measures created different clinical phenotypes of CRPS and possible CRPS subtypes, which distinguishes them from other CLP conditions, with the pro-inflammatory TNF-α cytokine as an additional potential biomarker.
复杂性区域疼痛综合征(CRPS)的分类已根据报告的亚型进行了更新,被定义为与其他慢性肢体疼痛(CLP)疾病并存的原发性疼痛。我们旨在确定能将CRPS与其他CLP疾病区分开来的CRPS临床表型。基于诱发疼痛(痛觉过敏强度、动态性痛觉过敏、痛觉过敏区域和后感觉)和心理(抑郁、运动恐惧、精神痛苦和人格解体)指标,对61例慢性CRPS患者和31例CLP患者进行聚类分析。检测促炎细胞因子白细胞介素-6(IL-6)和肿瘤坏死因子-α(TNF-α)的血清水平。创建了三个聚类组:“CRPS组”(78.7%为CRPS患者;6.5%为CLP患者);“CLP组”(64.5%为CLP患者;4.9%为CRPS患者)和“混合组”(16.4%为CRPS患者;29%为CLP患者)。这三组在所有指标上均存在差异,主要体现在痛觉过敏和痛觉超敏方面(p<0.001,η²>0.58)。与“CLP组”相比,“CRPS组”表现出更高的心理和诱发疼痛指标。“混合组”在心理特征上与“CRPS组”相似,在诱发疼痛指标上与“CLP组”相似。与“CLP组”相比,“CRPS组”的TNF-α血清水平更高(p<0.001)。总之,反映神经病理性疼痛机制的疼痛超敏和心理状态指标产生了CRPS不同的临床表型及可能的CRPS亚型,这使其有别于其他CLP疾病,促炎细胞因子TNF-α作为一种额外的潜在生物标志物。