Fan Chiang Yu-Hsuan, Wang Ming-Tse, Chan Shun-Ming, Chen Se-Yi, Wang Man-Ling, Hou Jin-De, Tsai Hsiao-Chien, Lin Jui-An
Department of Anesthesiology, Taipei Medical University Hospital, Taipei 11031, Taiwan.
Department of Anesthesiology, Tri-Service General Hospital and National Defense Medical Center, Taipei 11490, Taiwan.
Healthcare (Basel). 2023 Jan 10;11(2):210. doi: 10.3390/healthcare11020210.
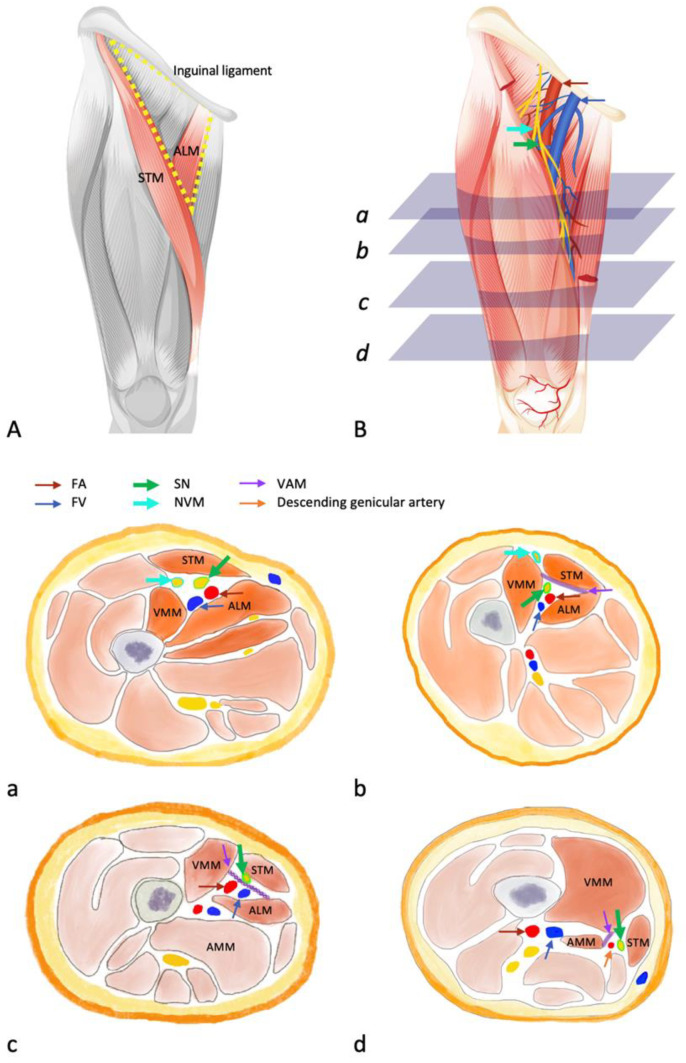
Discrepancies in the definition of adductor canal block (ACB) lead to inconsistent results. To investigate the actual analgesic and motor-sparing effects of ACB by anatomically defining femoral triangle block (FTB), proximal ACB (p-ACB), and distal ACB (d-ACB), we re-classified the previously claimed ACB approaches according to the ultrasound findings or descriptions in the corresponding published articles. A meta-analysis with subsequent subgroup analyses based on these corrected results was performed to examine the true impact of ACB on its analgesic effect and motor function (quadriceps muscle strength or mobilization ability). An optimal ACB technique was also suggested based on an updated review of evidence and ultrasound anatomy.
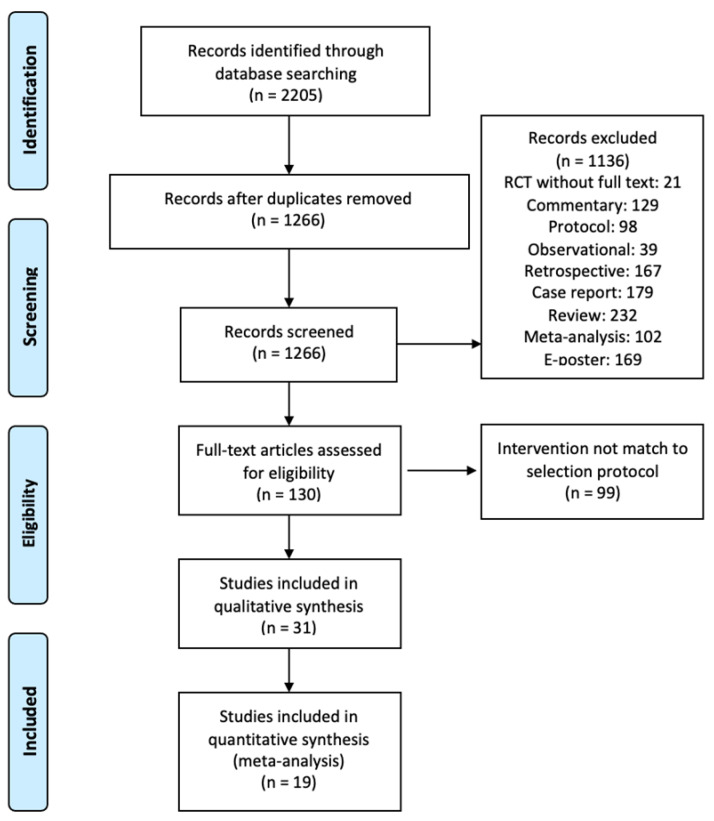
We systematically searched studies describing the use of ACB for knee surgery. Cochrane Library, PubMed, Web of Science, and Embase were searched with the exclusion of non-English articles from inception to 28 February 2022. The motor-sparing and analgesic aspects in true ACB were evaluated using meta-analyses with subsequent subgroup analyses according to the corrected classification system.
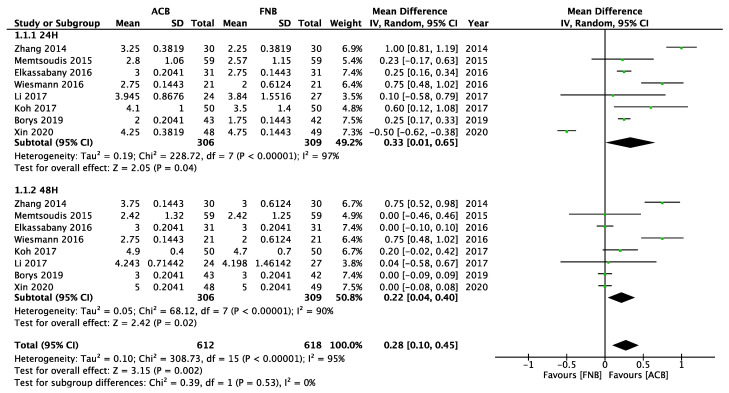
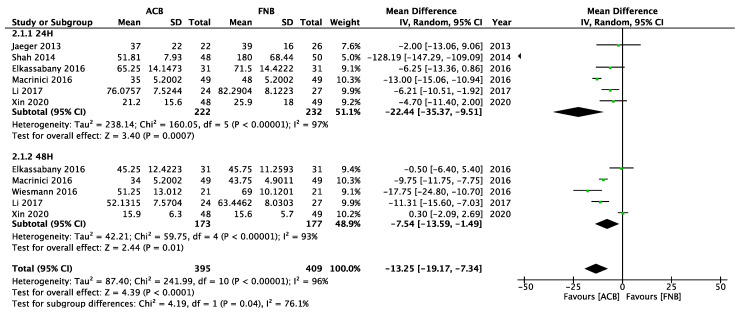
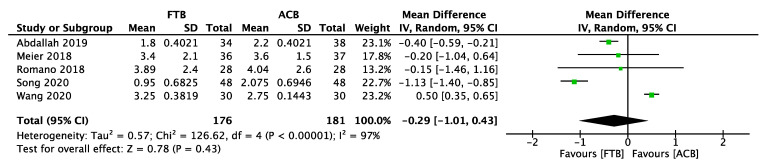
The meta-analysis includes 19 randomized controlled trials. Compared with the femoral nerve block group, the quadriceps muscle strength (standardized mean difference (SMD) = 0.33, 95%-CI [0.01; 0.65]) and mobilization ability (SMD = -22.44, 95%-CI [-35.37; -9.51]) are more preserved in the mixed ACB group at 24 h after knee surgery. Compared with the true ACB group, the FTB group (SMD = 5.59, 95%-CI [3.44; 8.46]) has a significantly decreased mobilization ability at 24 h after knee surgery.
By using the corrected classification system, we proved the motor-sparing effect of true ACB compared to FTB. According to the updated ultrasound anatomy, we suggested proximal ACB to be the analgesic technique of choice for knee surgery. Although a single-shot ACB is limited in duration, it remains the candidate of the analgesic standard for knee surgery on postoperative day 1 or 2 because it induces analgesia with less motor involvement in the era of multimodal analgesia. Furthermore, data from the corrected classification system may provide the basis for future research.
内收肌管阻滞(ACB)定义上的差异导致结果不一致。为了通过解剖学定义股三角阻滞(FTB)、近端ACB(p - ACB)和远端ACB(d - ACB)来研究ACB实际的镇痛和运动保留效果,我们根据超声检查结果或相应发表文章中的描述,对先前声称的ACB方法进行了重新分类。基于这些校正结果进行了荟萃分析及后续亚组分析,以检验ACB对其镇痛效果和运动功能(股四头肌力量或活动能力)的真实影响。还基于对证据和超声解剖学的更新回顾,提出了一种最佳的ACB技术。
我们系统检索了描述ACB用于膝关节手术的研究。检索了Cochrane图书馆、PubMed、科学网和Embase,排除了从创刊到2022年2月28日的非英文文章。根据校正后的分类系统,使用荟萃分析及后续亚组分析评估了真正ACB中的运动保留和镇痛方面。
荟萃分析纳入了19项随机对照试验。与股神经阻滞组相比,膝关节手术后24小时,混合ACB组的股四头肌力量(标准化均数差(SMD)= 0.33,95%可信区间[0.01;0.65])和活动能力(SMD = - 22.44,95%可信区间[- 35.37;- 9.51])保留得更好。与真正ACB组相比,FTB组在膝关节手术后24小时的活动能力显著下降(SMD = 5.59,95%可信区间[3.44;8.46])。
通过使用校正后的分类系统,我们证明了与FTB相比,真正ACB具有运动保留效果。根据更新后的超声解剖学,我们建议近端ACB是膝关节手术镇痛技术的首选。尽管单次ACB的持续时间有限,但在多模式镇痛时代,由于其引起的镇痛对运动的影响较小,它仍然是术后第1天或第2天膝关节手术镇痛标准的候选方法。此外,来自校正后分类系统的数据可能为未来的研究提供基础。