Department of Radiation Oncology, The First Affiliated Hospital of Xiamen University, Xiamen, China.
PLoS One. 2023 Jan 24;18(1):e0280456. doi: 10.1371/journal.pone.0280456. eCollection 2023.
Volumetric modulated arc therapy (VMAT) with varied bolus thicknesses has been employed in postmastectomy radiotherapy (PMRT) of breast cancer to improve superficial target coverage. However, impact of bolus thickness on plan robustness remains unclear.
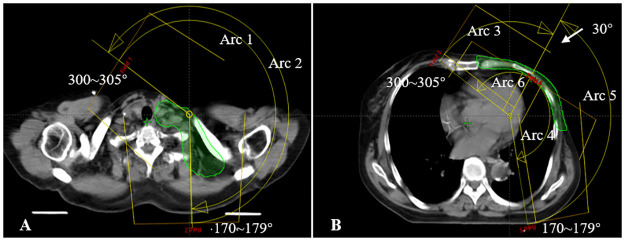
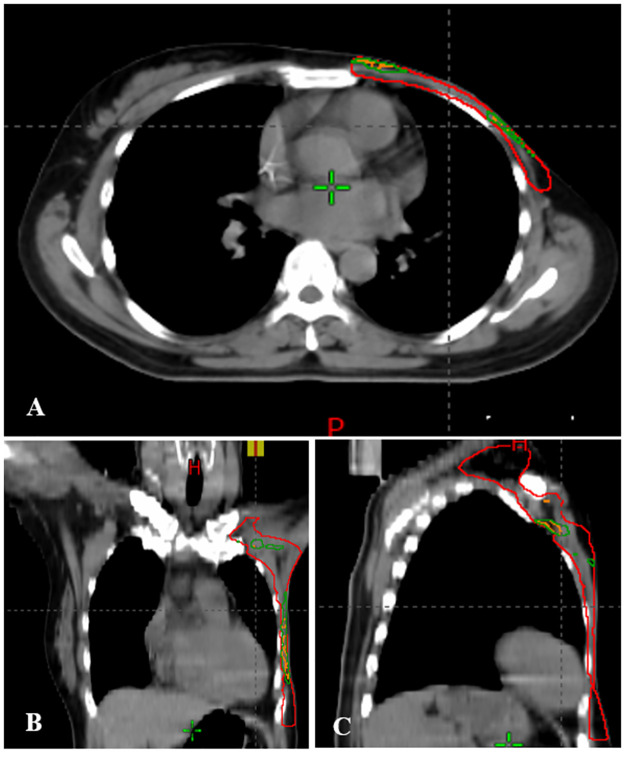
The study enrolled ten patients with left-sided breast cancer who received radiotherapy using VMAT with 5 mm and 10 mm bolus (VMAT-5B and VMAT-10B). Inter-fractional setup errors were simulated by introducing a 3 mm shift to isocenter of the original plans in the anterior-posterior, left-right, and inferior-superior directions. The plans (perturbed plans) were recalculated without changing other parameters. Dose volume histograms (DVH) were collected for plan evaluation. Absolute dose differences in DVH endpoints for the clinical target volume (CTV), heart, and left lung between the perturbed plans and the original ones were used for robustness analysis.
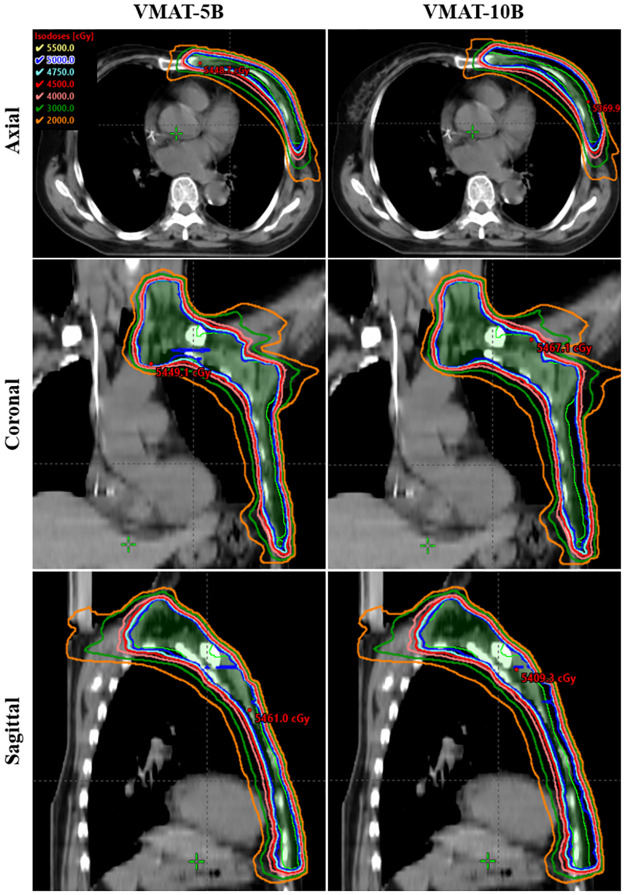
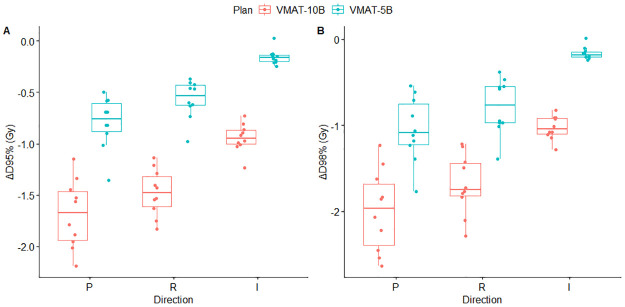
VMAT-10B showed better target coverage, while VMAT-5B was superior in organs-at-risk (OARs) sparing. As expected, small setup errors of 3 mm could induce dose fluctuations in CTV and OARs. The differences in CTV were small in VMAT-5B, with a maximum difference of -1.05 Gy for the posterior shifts. For VMAT-10B, isocenter shifts in the posterior and right directions significantly decreased CTV coverage. The differences were -1.69 Gy, -1.48 Gy and -1.99 Gy, -1.69 Gy for ΔD95% and ΔD98%, respectively. Regarding the OARs, only isocenter shifts in the posterior, right, and inferior directions increased dose to the left lung and the heart. Differences in VMAT-10B were milder than those in VMAT-5B. Specifically, mean heart dose were increased by 0.42 Gy (range 0.10 ~ 0.95 Gy) and 0.20 Gy (range -0.11 ~ 0.72 Gy), and mean dose for the left lung were increased by 1.02 Gy (range 0.79 ~ 1.18 Gy) and 0.68 Gy (range 0.47 ~ 0.84 Gy) in VMAT-5B and VMAT-10B, respectively. High-dose volumes in the organs were increased by approximate 0 ~ 2 and 1 ~ 3 percentage points, respectively. Nevertheless, most of the dosimetric parameters in the perturbed plans were still clinically acceptable.
VMAT-5B appears to be more robust to 3 mm setup errors than VMAT-10B. VMAT-5B also resulted in better OARs sparing with acceptable target coverage and dose homogeneity. Therefore 5 mm bolus is recommended for PMRT of left-sided breast cancer using VMAT.
在乳腺癌根治术后放疗(PMRT)中,采用变厚楔形板的容积调强弧形治疗(VMAT)已被用于改善浅表靶区覆盖。然而,楔形板厚度对计划稳健性的影响仍不清楚。
本研究纳入了 10 例接受 VMAT 治疗的左侧乳腺癌患者,VMAT 分别采用 5mm(VMAT-5B)和 10mm(VMAT-10B)楔形板。通过在前后、左右和上下方向上向原始计划的等中心引入 3mm 的偏移来模拟分次间摆位误差。在不改变其他参数的情况下,重新计算计划(受扰计划)。收集剂量体积直方图(DVH)进行计划评估。受扰计划与原始计划之间临床靶区(CTV)、心脏和左肺的 DVH 终点的绝对剂量差异用于稳健性分析。
VMAT-10B 显示出更好的靶区覆盖,而 VMAT-5B 在保护危及器官(OARs)方面更有优势。如预期的那样,3mm 的小摆位误差会导致 CTV 和 OAR 中的剂量波动。在 VMAT-5B 中,CTV 的差异较小,后向移位的最大差异为-1.05Gy。对于 VMAT-10B,后向和右侧的等中心移位显著降低了 CTV 的覆盖范围。差异分别为-1.69Gy、-1.48Gy 和-1.99Gy、-1.69Gy,用于ΔD95%和ΔD98%。对于 OARs,只有后向、右侧和下方的等中心移位会增加左肺和心脏的剂量。VMAT-10B 的差异比 VMAT-5B 更轻微。具体而言,VMAT-5B 中心脏的平均剂量增加了 0.42Gy(范围 0.100.95Gy)和 0.20Gy(范围-0.110.72Gy),而左肺的平均剂量增加了 1.02Gy(范围 0.791.18Gy)和 0.68Gy(范围 0.470.84Gy)。器官的高剂量体积分别增加了约 02%和 13%。然而,受扰计划中的大多数剂量学参数仍然是临床可接受的。
与 VMAT-10B 相比,VMAT-5B 似乎对 3mm 的摆位误差更稳健。VMAT-5B 还具有更好的 OAR 保护作用,同时具有可接受的靶区覆盖范围和剂量均匀性。因此,在左侧乳腺癌的 VMAT 治疗中,建议使用 5mm 楔形板。