Department of Neurology, Hospital of the University of Pennsylvania, Philadelphia.
Center for Population Health Sciences, Stanford University, Palo Alto, California.
JAMA Netw Open. 2023 Jan 3;6(1):e2252689. doi: 10.1001/jamanetworkopen.2022.52689.
Psychosis is a hypothesized consequence of cannabis use. Legalization of cannabis could therefore be associated with an increase in rates of health care utilization for psychosis.
To evaluate the association of state medical and recreational cannabis laws and commercialization with rates of psychosis-related health care utilization.
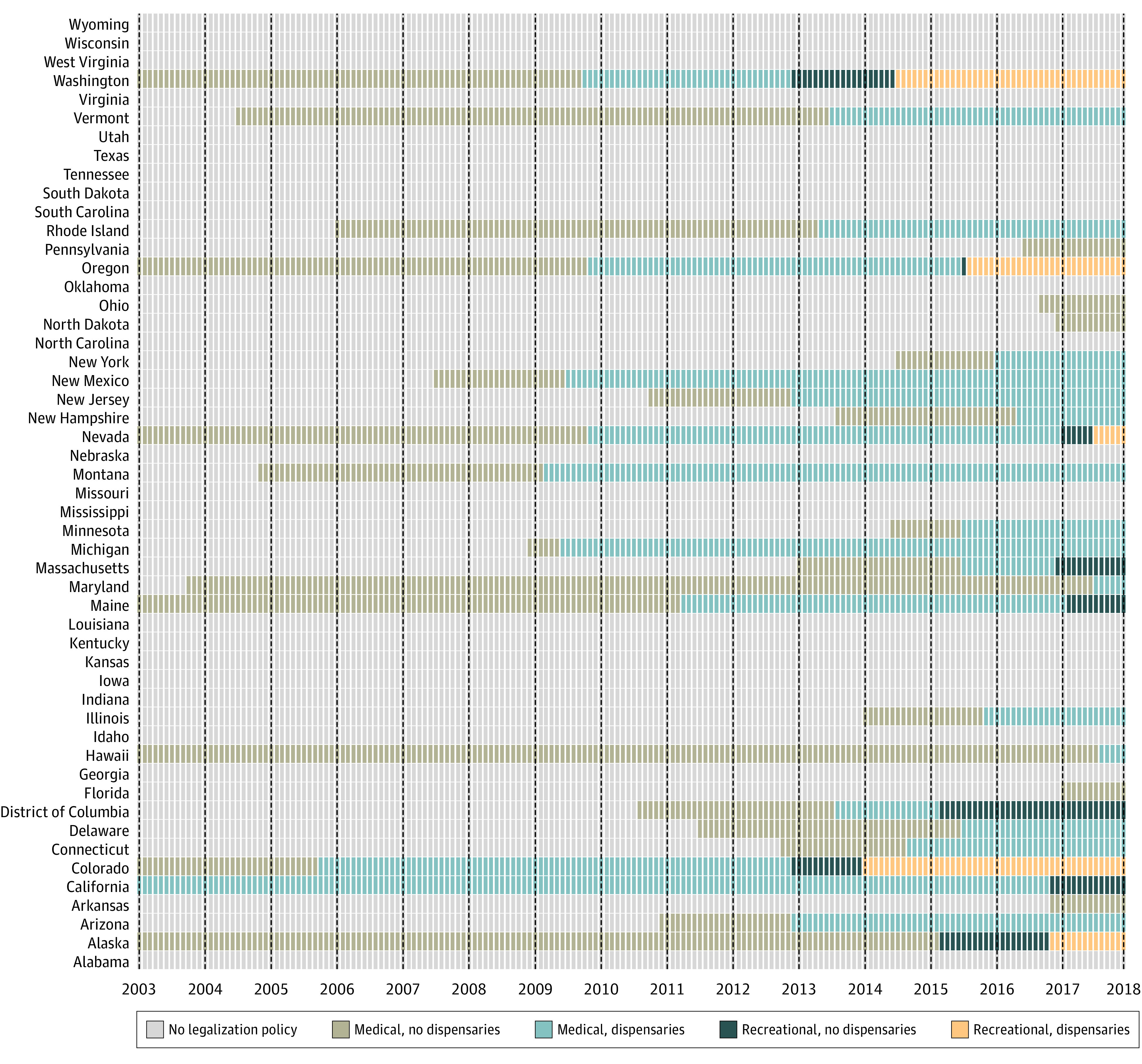
DESIGN, SETTING, AND PARTICIPANTS: Retrospective cohort design using state-level panel fixed effects to model within-state changes in monthly rates of psychosis-related health care claims as a function of state cannabis policy level, adjusting for time-varying state-level characteristics and state, year, and month fixed effects. Commercial and Medicare Advantage claims data for beneficiaries aged 16 years and older in all 50 US states and the District of Columbia, 2003 to 2017 were used. Data were analyzed from April 2021 to October 2022.
State cannabis legalization policies were measured for each state and month based on law type (medical or recreational) and degree of commercialization (presence or absence of retail outlets).
Outcomes were rates of psychosis-related diagnoses and prescribed antipsychotics.
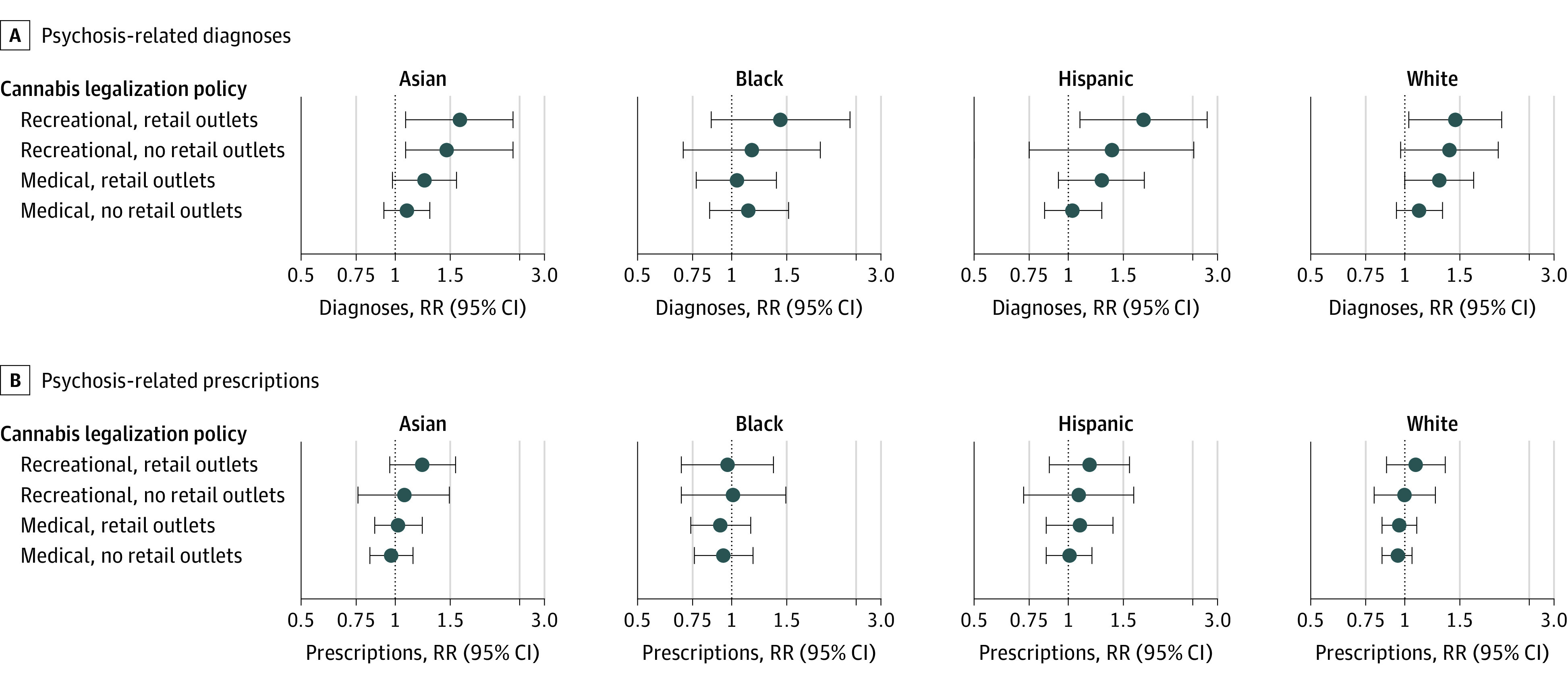
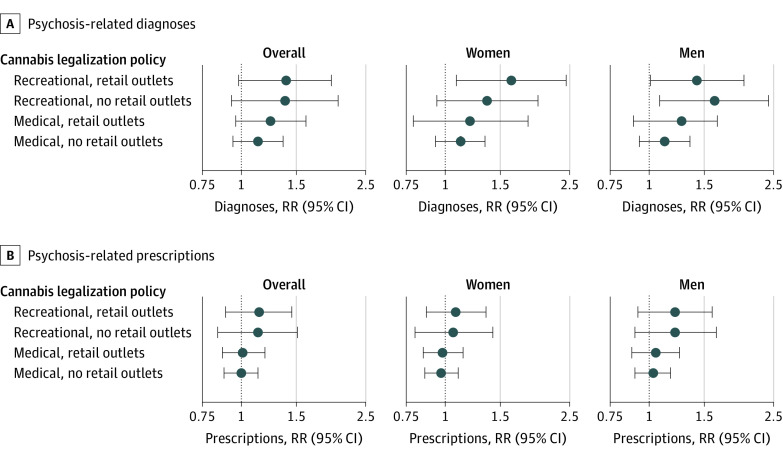
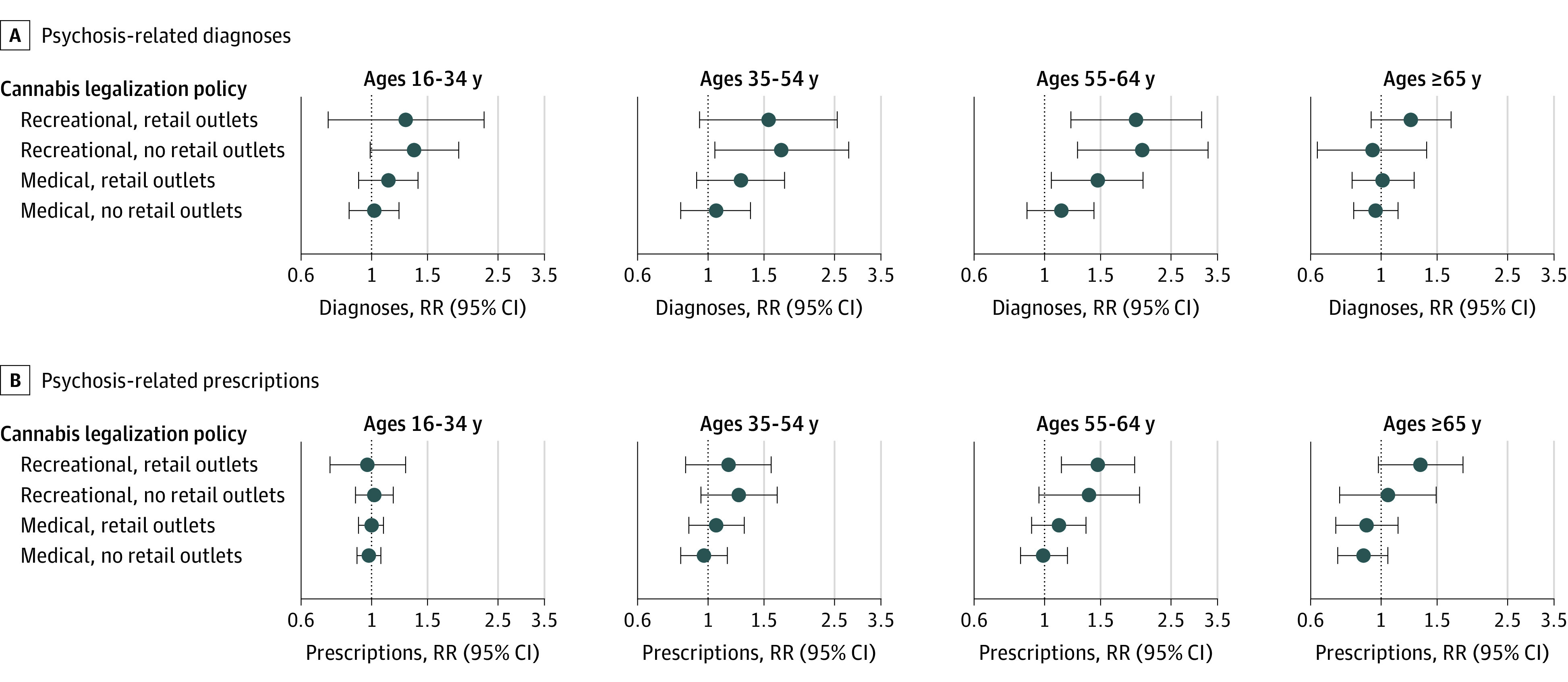
This study included 63 680 589 beneficiaries followed for 2 015 189 706 person-months. Women accounted for 51.8% of follow-up time with the majority of person-months recorded for those aged 65 years and older (77.3%) and among White beneficiaries (64.6%). Results from fully-adjusted models showed that, compared with no legalization policy, states with legalization policies experienced no statistically significant increase in rates of psychosis-related diagnoses (medical, no retail outlets: rate ratio [RR], 1.13; 95% CI, 0.97-1.36; medical, retail outlets: RR, 1.24; 95% CI, 0.96-1.61; recreational, no retail outlets: RR, 1.38; 95% CI, 0.93-2.04; recreational, retail outlets: RR, 1.39; 95% CI, 0.98-1.97) or prescribed antipsychotics (medical, no retail outlets RR, 1.00; 95% CI, 0.88-1.13; medical, retail outlets: RR, 1.01; 95% CI, 0.87-1.19; recreational, no retail outlets: RR, 1.13; 95% CI, 0.84-1.51; recreational, retail outlets: RR, 1.14; 95% CI, 0.89-1.45). In exploratory secondary analyses, rates of psychosis-related diagnoses increased significantly among men, people aged 55 to 64 years, and Asian beneficiaries in states with recreational policies compared with no policy.
In this retrospective cohort study of commercial and Medicare Advantage claims data, state medical and recreational cannabis policies were not associated with a statistically significant increase in rates of psychosis-related health outcomes. As states continue to introduce new cannabis policies, continued evaluation of psychosis as a potential consequence of state cannabis legalization may be informative.
精神病是使用大麻的假设后果。因此,大麻合法化可能与精神疾病相关的医疗保健利用率的增加有关。
评估州医疗和娱乐性大麻法律以及商业化与精神病相关的医疗保健利用率之间的关联。
设计、地点和参与者:使用州级面板固定效应进行回顾性队列设计,根据州大麻政策水平,对每月精神病相关医疗保健索赔率的变化进行建模,同时调整了随时间变化的州级特征以及州、年和月固定效应。使用了美国所有 50 个州和哥伦比亚特区 16 岁及以上的商业和医疗保险优势索赔数据,时间范围为 2003 年至 2017 年。数据分析于 2021 年 4 月至 2022 年 10 月进行。
根据法律类型(医疗或娱乐)和商业化程度(是否有零售店),对每个州和每个月的州大麻合法化政策进行测量。
结果是精神病相关诊断和处方抗精神病药物的比率。
本研究纳入了 63680589 名被随访者,随访时间为 2015189706 人月。女性占随访时间的 51.8%,记录的大多数人月是 65 岁及以上的人(77.3%)和白人被随访者(64.6%)。完全调整模型的结果显示,与没有合法化政策的州相比,有合法化政策的州在精神病相关诊断率(医疗,无零售:比率比 [RR],1.13;95%CI,0.97-1.36;医疗,有零售:RR,1.24;95%CI,0.96-1.61;娱乐,无零售:RR,1.38;95%CI,0.93-2.04;娱乐,有零售:RR,1.39;95%CI,0.98-1.97)或处方抗精神病药物率(医疗,无零售:RR,1.00;95%CI,0.88-1.13;医疗,有零售:RR,1.01;95%CI,0.87-1.19;娱乐,无零售:RR,1.13;95%CI,0.84-1.51;娱乐,有零售:RR,1.14;95%CI,0.89-1.45)方面并没有统计学上的显著增加。在探索性的次要分析中,与没有政策的州相比,有娱乐性政策的州中,男性、55 岁至 64 岁的人和亚洲裔被随访者的精神病相关诊断率显著增加。
在这项对商业和医疗保险优势索赔数据的回顾性队列研究中,州医疗和娱乐性大麻政策与精神病相关医疗结果的发生率没有统计学上的显著增加。随着各州继续引入新的大麻政策,对精神病作为州大麻合法化的潜在后果的持续评估可能会有所帮助。