Tsolaki Vasiliki, Aravantinou-Fatorou Aikaterini, Georgakopoulou Vasiliki Epameinondas, Spandidos Demetrios A, Papalexis Petros, Mathioudakis Nikolaos, Tarantinos Kyriakos, Trakas Nikolaos, Sklapani Pagona, Fotakopoulos George
Department of Pulmonary and Critical Care Medicine, General University Hospital of Larisa, 41221 Larisa, Greece.
First Department of Internal Medicine, Laiko General Hospital, Medical School, National and Kapodistrian University of Athens, 11527 Athens, Greece.
Med Int (Lond). 2022 Nov 2;2(6):34. doi: 10.3892/mi.2022.59. eCollection 2022 Nov-Dec.
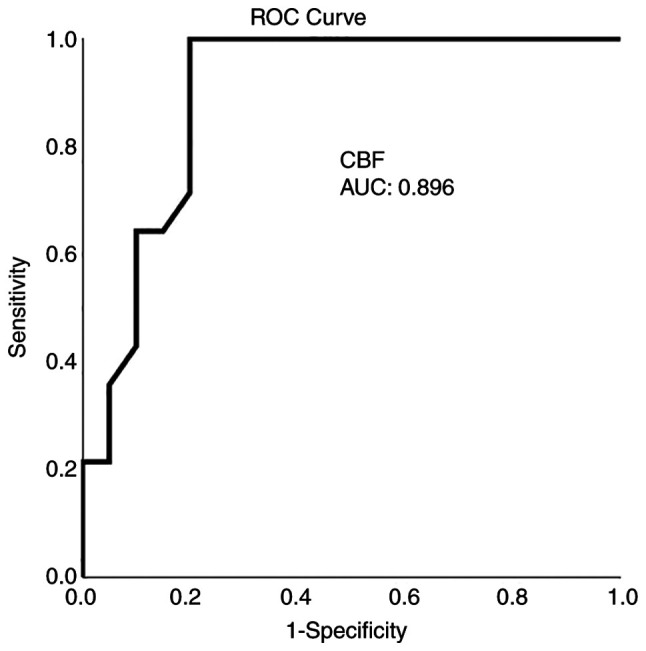
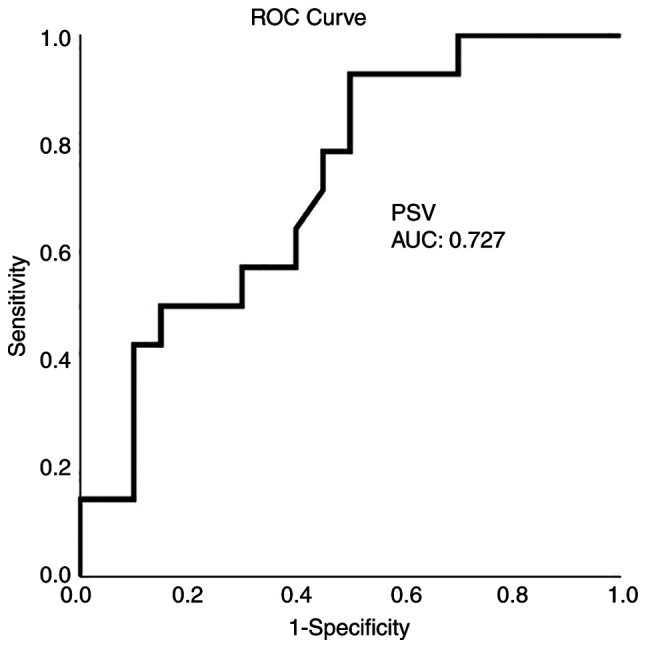
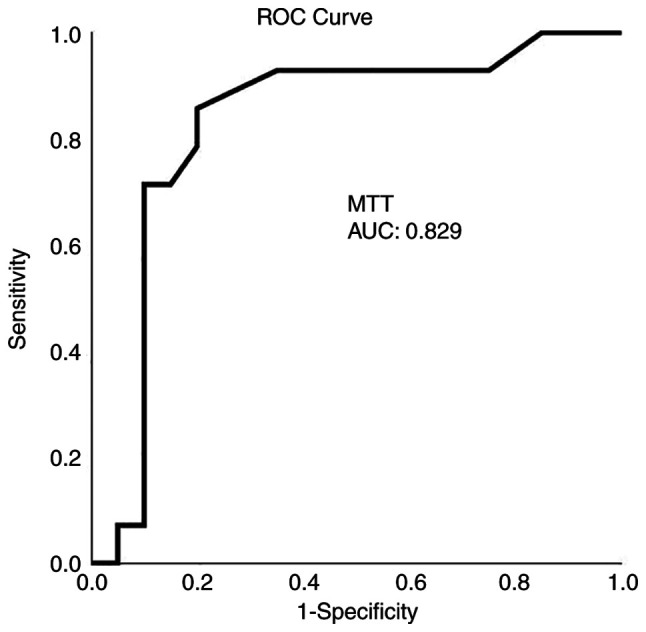
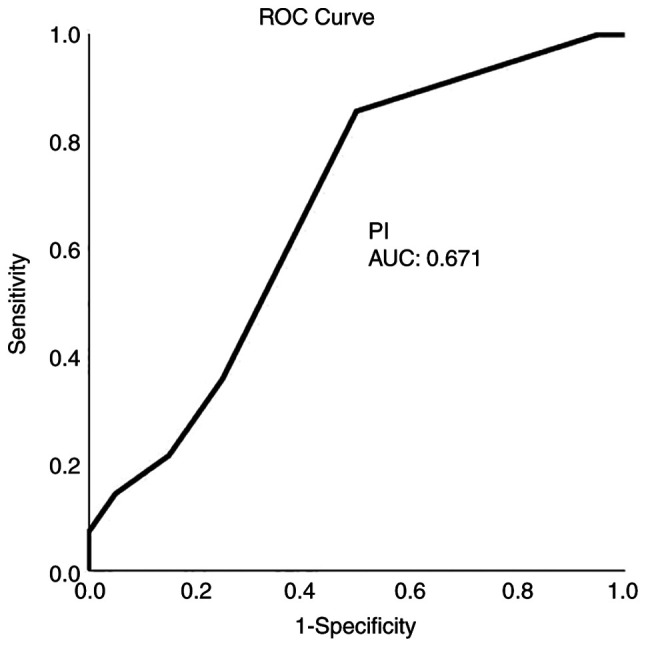
Cerebral vasospasm (CV) constitutes a major post-operative complication and source of morbidity in cases of subarachnoid hemorrhage (SAH). The early detection of CV in SAH may be difficult both clinically and radiographically. The present pilot study thus aimed to evaluate the practicability of the technique in a tertiary healthcare setting and to assess the diagnostic effectiveness of various diagnostic computed tomography (CT) perfusion (CTP) aspects in predicting the clinical outcome of patients with SAH (traumatic and aneurysmal). A retrospective study including 34 patients in a tertiary care hospital was thus conducted. The results revealed that of the 34 patients, 18 (52.9%) were males, and the mean age was 54.4±18.5 years (16-85 years old; range, 69 years). In total, 15 (44.1%) patients had traumatic SAH following traumatic brain injury (TBI), 11 (33.3%) had aneurysmal SAH, and 8 patients (23.6%) presented with TBI without SAH as controls. CTP was performed on the third to the sixth day, and 15-20 min prior to CPT, a transcranial Doppler ultrasound was performed. Clinical outcomes were documented at 30 days using a CT scan and a complete neurological evaluation, including Glasgow Coma Scale assessment. The results of a multivariate analysis revealed that cerebral blood flow (CBF) was an independent factor for detecting an ischemic event in 1 month (P=0.003). On the whole, the present study demonstrates that CTP, and consequently CBF, is a considerable index that may identify the onset of cerebral ischemia in patients with SAH.
脑血管痉挛(CV)是蛛网膜下腔出血(SAH)病例中的一种主要术后并发症和发病源。SAH中CV的早期检测在临床和影像学上都可能很困难。因此,本初步研究旨在评估该技术在三级医疗环境中的实用性,并评估各种诊断性计算机断层扫描(CT)灌注(CTP)方面在预测SAH(创伤性和动脉瘤性)患者临床结局方面的诊断有效性。因此,在一家三级护理医院进行了一项包括34例患者的回顾性研究。结果显示,在这34例患者中,18例(52.9%)为男性,平均年龄为54.4±18.5岁(16 - 85岁;范围为69岁)。总共有15例(44.1%)患者在创伤性脑损伤(TBI)后发生创伤性SAH,11例(33.3%)有动脉瘤性SAH,8例患者(23.6%)表现为TBI但无SAH作为对照。在第3至6天进行CTP检查,在CTP检查前15 - 20分钟进行经颅多普勒超声检查。使用CT扫描和包括格拉斯哥昏迷量表评估在内的完整神经学评估在30天时记录临床结局。多变量分析结果显示,脑血流量(CBF)是检测1个月内缺血事件的独立因素(P = 0.003)。总体而言,本研究表明CTP,进而CBF,是一个重要指标,可能识别SAH患者脑缺血的发作。