Population Health Sciences, University of Bristol, Bristol, UK.
Department of Global HIV, Hepatitis and STI Programmes, World Health Organization, Geneva, Switzerland.
Lancet Gastroenterol Hepatol. 2023 Mar;8(3):253-270. doi: 10.1016/S2468-1253(22)00346-6. Epub 2023 Jan 24.
Point-of-care (POC) hepatitis C virus (HCV) RNA nucleic acid test viral load assays are being used increasingly as an alternative to centralised, laboratory-based standard-of-care (SOC) viral load assays to reduce loss to follow-up. We aimed to evaluate the impact of using POC compared with SOC approaches on uptake of HCV RNA viral load testing and treatment, and turnaround times from testing to treatment along the HCV care cascade.
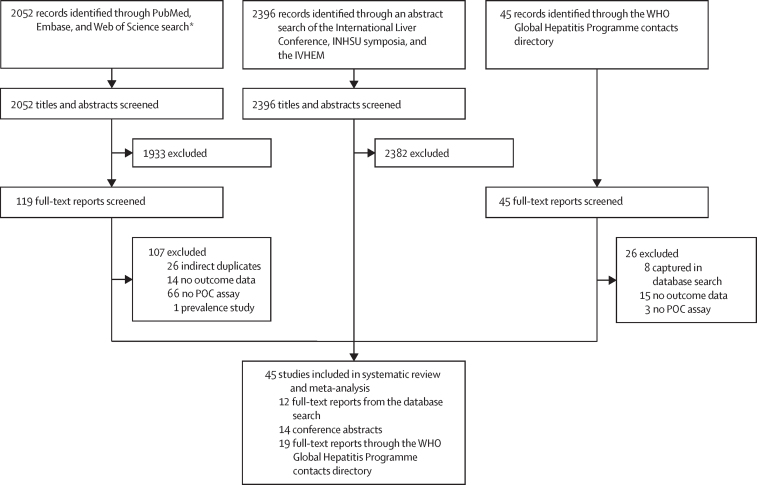
We searched PubMed, Embase, and Web of Science for studies published in English between Jan 1, 2016, and April 13, 2022. We additionally searched for accepted conference abstracts (2016-20) not identified in the main search. The contacts directory of the WHO Global Hepatitis Programme was also used to solicit additional studies on use of POC RNA assays. We included studies if they evaluated use of POC HCV RNA viral load with or without a comparator laboratory-based SOC assay, and had data on uptake of viral load testing and treatment, and turnaround times between these steps in cascade. We excluded studies with a sample size of ten or fewer participants. The POC studies were categorised according to whether the POC assay was based onsite at the clinic, in a mobile unit, or in a laboratory. Studies using the POC assay or comparator SOC assays were further stratified according to four models of care: whether HCV testing and treatment initiation were performed in the same or different site, and on the same or a different visit. The comparator was centralised, laboratory-based HCV RNA SOC assays. For turnaround times, we calculated the weighted median of medians with 95% CIs. We analysed viral load testing and treatment uptake using random-effects meta-analysis. The quality of evidence was rated using the GRADE framework. This study is registered with PROSPERO, CRD42020218239.
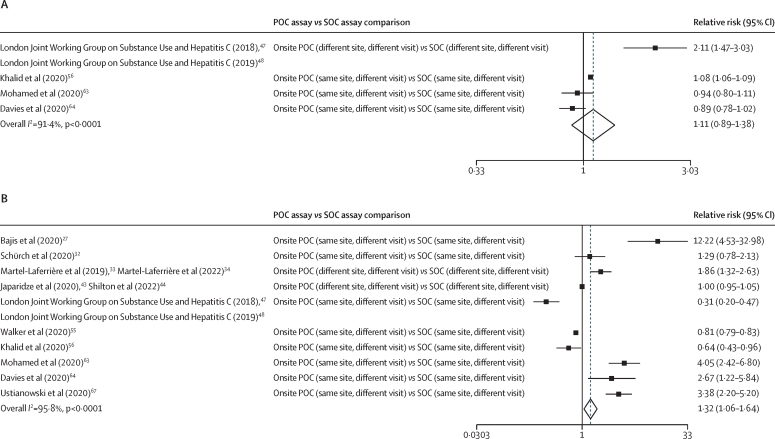
We included 45 studies with 64 within-study arms: 28 studies were in people who inject drugs, were homeless, or both; four were in people incarcerated in prison; nine were in the general or mixed (ie, includes high-risk groups) populations; and four were in people living with HIV. All were observational studies. The pooled median turnaround times between HCV antibody test and treatment initiation was shorter with onsite POC assays (19 days [95% CI 14-53], ten arms) than with either laboratory-based POC assays (64 days [64-64], one arm) or laboratory-based SOC assays (67 days [50-67], two arms). Treatment uptake was higher with onsite POC assays (77% [95% CI 72-83], 34 arms) or mobile POC assays (81% [60-97], five arms) than with SOC assays (53% [31-75], 12 arms); onsite and mobile POC assay vs SOC assay p=0·029). For POC and SOC arms, higher RNA viral load testing uptake was seen with the same-site models for testing and treatment than with different-site models (all within-category p≤0·0001). For onsite and mobile POC arms, there was higher treatment uptake for same-site than different-site models (within-category p<0·0001). Four studies had direct within-study POC versus SOC comparisons for RNA viral load testing uptake (pooled relative risk 1·11 [95% CI 0·89-1·38]), and there were ten studies on treatment uptake (1·32 [1·06-1·64]). Overall, the quality of evidence was rated as low.
Compared with use of laboratory-based SOC HCV viral load testing, the use of POC assays was associated with reduced time from antibody test to treatment initiation and increased treatment uptake. The effect of POC viral load testing is greatest when positioned within a simplified care model in which testing and treatment are provided at the same site, and, where possible, on the same day. POC HCV RNA viral load testing is now recommended in WHO guidelines as an alternative strategy to laboratory-based viral load testing.
Unitaid.
即时检测(POC)丙型肝炎病毒(HCV)RNA 核酸检测病毒载量分析正越来越多地被用作替代集中式、基于实验室的标准治疗(SOC)病毒载量分析的方法,以减少失访。我们旨在评估与 SOC 方法相比,使用 POC 对 HCV RNA 病毒载量检测和治疗的影响,以及从检测到治疗沿 HCV 护理级联的周转时间。
我们在 PubMed、Embase 和 Web of Science 上搜索了 2016 年 1 月 1 日至 2022 年 4 月 13 日期间发表的英文研究。我们还额外搜索了 2016-20 年未在主要搜索中确定的接受会议摘要。世界卫生组织全球肝炎计划的联系人目录也被用来征求更多关于使用 POC RNA 检测的研究。如果研究评估了使用 POC HCV RNA 病毒载量检测与或不与基于实验室的 SOC 检测进行比较,并且有关于病毒载量检测和治疗的接受率以及级联中这些步骤之间的周转时间的数据,则将其纳入研究。我们排除了样本量为 10 或更少参与者的研究。根据 POC 检测是在诊所现场、移动单位还是实验室进行,将 POC 研究分类。根据 HCV 检测和治疗启动是否在同一地点或不同地点进行,以及在同一或不同访问进行,将使用 POC 检测或比较 SOC 检测的研究进一步分层。比较器是集中式、基于实验室的 HCV RNA SOC 检测。对于周转时间,我们计算了中值的加权中位数和 95%CI。我们使用随机效应荟萃分析分析了病毒载量检测和治疗的接受率。使用 GRADE 框架评估证据质量。这项研究在 PROSPERO 上注册,注册号为 CRD42020218239。
我们纳入了 45 项研究,共 64 项研究臂:28 项研究涉及注射毒品者、无家可归者或两者兼有;四项研究涉及被监禁的囚犯;九项研究涉及一般或混合人群(即包括高风险人群);四项研究涉及 HIV 感染者。所有研究均为观察性研究。与基于实验室的 SOC 检测相比,现场 POC 检测(19 天[95%CI 14-53],10 个臂)的 HCV 抗体检测和治疗启动之间的周转时间更短,而基于实验室的 POC 检测(64 天[64-64],一个臂)或基于实验室的 SOC 检测(67 天[50-67],两个臂)。现场 POC 检测(77%[95%CI 72-83],34 个臂)或移动 POC 检测(81%[60-97],5 个臂)的治疗接受率高于 SOC 检测(53%[31-75],12 个臂);现场和移动 POC 检测与 SOC 检测的 p 值为 0.029)。对于 POC 和 SOC 臂,与不同地点模型相比,同一地点模型的 HCV RNA 病毒载量检测接受率更高(所有分类内 p 值均≤0.0001)。对于现场和移动 POC 臂,同一地点模型的治疗接受率高于不同地点模型(分类内 p 值均<0.0001)。四项研究对 POC 与 SOC 进行了直接的病毒载量检测比较(汇总相对风险 1.11[95%CI 0.89-1.38]),十项研究对治疗接受率进行了比较(1.32[1.06-1.64])。总体而言,证据质量被评为低。
与使用基于实验室的 SOC HCV 病毒载量检测相比,使用 POC 检测与缩短从抗体检测到治疗启动的时间和提高治疗接受率有关。当 POC 病毒载量检测在简化的护理模型中定位时,其效果最大,在该模型中,检测和治疗都在同一地点进行,并且在可能的情况下在同一天进行。POC HCV RNA 病毒载量检测现已被世界卫生组织指南推荐为替代基于实验室的病毒载量检测的一种策略。
联合国艾滋病规划署。