Foundation for Innovative New Diagnostics, Geneva, Switzerland.
US Centers for Disease Control and Prevention, Atlanta, Georgia, USA.
Liver Int. 2022 Apr;42(4):775-786. doi: 10.1111/liv.15191. Epub 2022 Feb 18.
In 2015, Georgia began a hepatitis C virus (HCV) elimination programme. Although screening programmes have been decentralized for high-risk groups, viraemic testing remains a bottleneck for people who inject drugs. Here, we describe two models of viraemic testing that aimed to address this gap.
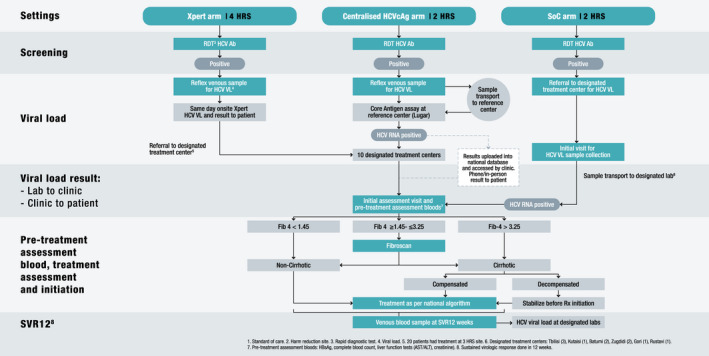
We assigned eight harm reduction sites (HRS) to one of three arms (2,1:1): Xpert HCV viral load testing on-site, blood draw on-site with centralized HCV core antigen testing (HCVcAg), or standard-of-care (SOC) referral with viremia testing performed at treatment centres.
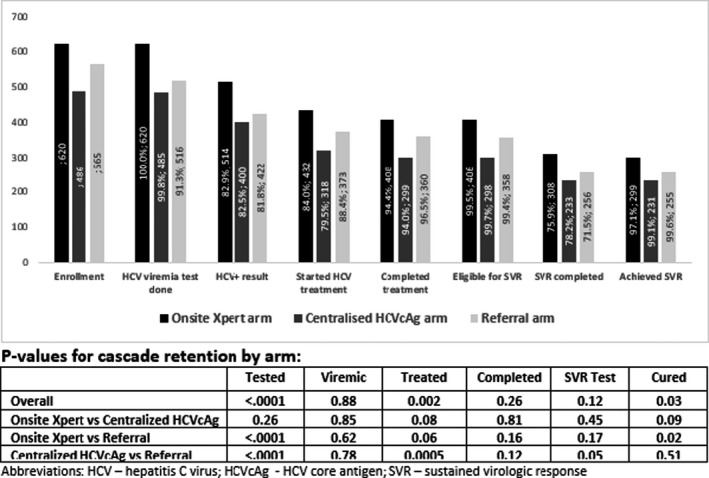
1671 HCV-seropositive participants were enrolled (Xpert, 37.1%; HCVcAg, 29.1%; referral, 33.8%). Participants were predominantly male (95.4%), mean age (IQR) 43 (37, 50) years and 1290 (77.2%) were currently injecting drugs. Significantly higher proportions of participants in the Xpert (100%) and HCVcAg (99.8%) arms received viraemia testing compared with the referral arm (91.3%) (Xpert vs referral, p < 0.0001; HCVcAg vs referral, p < 0.0001). Among viraemic participants, treatment uptake was similar (Xpert, 84.0%; HCVcAg, 79.5%; referral, 88.4%). The time between screening and sample collection for viraemia testing was significantly longer in the referral arm compared with both Xpert and HCVcAg arms (median 1 day compared with 0 days respectively), and the overall time between screening to treatment initiation was longer for the referral arm (median 67 days) compared with both Xpert and HCVcAg arms (median 57 and 50 days respectively).
Point-of-care viraemia testing and blood drawn on-site for HCVcAg testing yielded more HCV-seropositive patients receiving viraemic testing within a shorter timeframe compared with referrals.
2015 年,格鲁吉亚启动了丙型肝炎病毒(HCV)消除计划。虽然筛查计划已经针对高危人群去中心化,但对于注射毒品的人来说,病毒血症检测仍然是一个瓶颈。在这里,我们描述了两种旨在解决这一差距的病毒血症检测模型。
我们将八个减少伤害场所(HRS)分配到三个臂中的一个(2,1:1):现场 Xpert HCV 病毒载量检测、现场采血和集中 HCV 核心抗原检测(HCVcAg),或标准护理(SOC)转介,病毒血症检测在治疗中心进行。
共纳入 1671 名 HCV 血清阳性参与者(Xpert,37.1%;HCVcAg,29.1%;转介,33.8%)。参与者主要为男性(95.4%),平均年龄(IQR)为 43(37,50)岁,1290 名(77.2%)目前正在注射毒品。与转介臂相比,Xpert(100%)和 HCVcAg(99.8%)臂的参与者接受病毒血症检测的比例显著更高(Xpert 与转介,p<0.0001;HCVcAg 与转介,p<0.0001)。在病毒血症阳性的参与者中,治疗吸收率相似(Xpert,84.0%;HCVcAg,79.5%;转介,88.4%)。与 Xpert 和 HCVcAg 臂相比,转介臂的病毒血症检测样本采集时间明显更长(中位数分别为 1 天和 0 天),转介臂从筛查到治疗开始的总时间也更长(中位数为 67 天),Xpert 和 HCVcAg 臂分别为 57 天和 50 天。
现场病毒血症检测和现场采血进行 HCVcAg 检测,与转介相比,在更短的时间内使更多 HCV 血清阳性患者接受病毒血症检测。