Disease Elimination Program, Burnet Institute, Melbourne, Australia.
School of Public Health and Preventive Medicine, Monash University, Melbourne, Australia.
Liver Int. 2021 Nov;41(11):2578-2589. doi: 10.1111/liv.14983. Epub 2021 Jul 10.
With the advent of low-cost generic direct-acting antivirals (DAA), hepatitis C (HCV) elimination is now achievable even in low-/middle-income settings. We assessed the feasibility and effectiveness of a simplified clinical pathway using point-of-care diagnostic testing and non-specialist-led care in a decentralized, community-based setting.
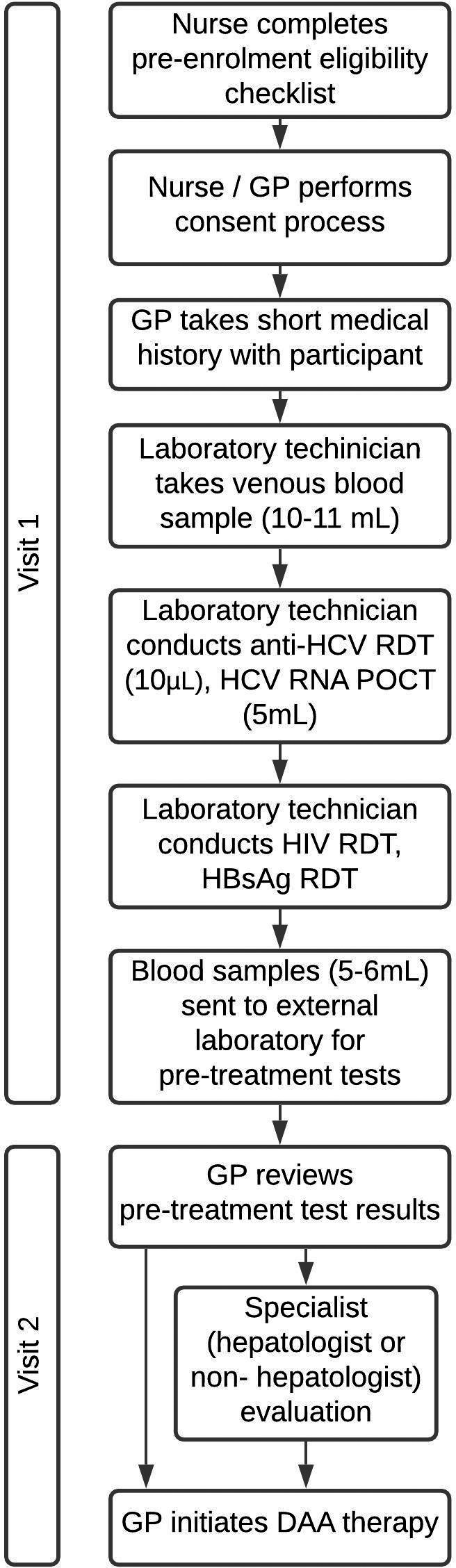
This feasibility study was conducted at two sites in Yangon, Myanmar: one for people who inject drugs (PWID), and the other for people with liver disease. Participants underwent on-site rapid anti-HCV testing and HCV RNA testing using GeneXpert . General practitioners determined whether participants started DAA therapy immediately or required specialist evaluation. Primary outcome measures were progression through the HCV care cascade, including uptake of RNA testing and treatment, and treatment outcomes.
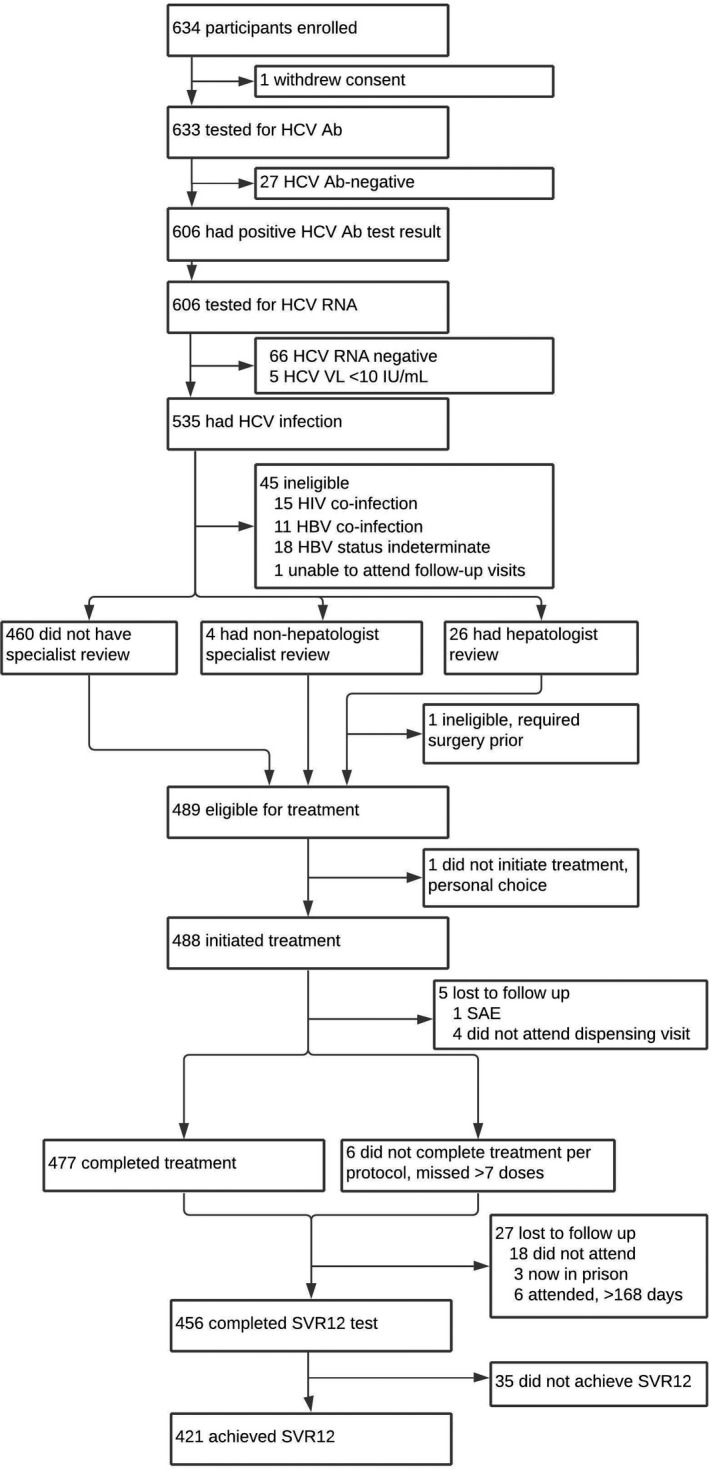
All 633 participants underwent anti-HCV testing; 606 (96%) were anti-HCV positive and had HCV RNA testing. Of 606 tested, 535 (88%) were RNA positive and had pre-treatment assessments; 30 (6%) completed specialist evaluation. Of 535 RNA positive participants, 489 (91%) were eligible to initiate DAAs, 477 (98%) completed DAA therapy and 421 achieved SVR12 (92%; 421/456). Outcomes were similar by site: PWID site: 91% [146/161], and liver disease site: 93% [275/295]). Compensated cirrhotic patients were treated in the community; they achieved an SVR12 of 83% (19/23). Median time from RNA test to DAA initiation was 3 days (IQR 2-5).
Delivering a simplified, non-specialist-led HCV treatment pathway in a decentralized community setting was feasible in Yangon, Myanmar; retention in care and treatment success rates were very high. This care model could be integral in scaling up HCV services in Myanmar and other low- and middle-income settings.
随着廉价通用直接作用抗病毒药物(DAA)的出现,即使在低收入/中等收入国家,丙型肝炎(HCV)也可以消除。我们评估了在分散的社区环境中使用即时检测诊断测试和非专科医生主导的护理的简化临床路径的可行性和有效性。
这项可行性研究在缅甸仰光的两个地点进行:一个针对注射吸毒者(PWID),另一个针对肝病患者。参与者接受现场快速抗 HCV 测试和 GeneXpert HCV RNA 测试。全科医生确定参与者是否立即开始 DAA 治疗,还是需要专家评估。主要结果衡量标准是 HCV 护理级联的进展情况,包括 RNA 检测和治疗的接受情况以及治疗结果。
所有 633 名参与者均接受了抗 HCV 检测;606(96%)名抗 HCV 阳性且接受 HCV RNA 检测。在 606 名接受检测的人中,535(88%)名 RNA 阳性且进行了治疗前评估;30(6%)名完成了专家评估。在 535 名 RNA 阳性的参与者中,489(91%)名符合 DAA 治疗标准,477(98%)名完成 DAA 治疗,421 名获得 SVR12(92%;421/456)。两个地点的结果相似:PWID 地点:91%[146/161],肝病地点:93%[275/295])。代偿性肝硬化患者在社区中接受治疗;他们获得了 83%(19/23)的 SVR12。从 RNA 检测到 DAA 开始的中位时间为 3 天(IQR 2-5)。
在缅甸仰光,在分散的社区环境中提供简化的、非专科医生主导的 HCV 治疗途径是可行的;护理保留率和治疗成功率非常高。这种护理模式可能是在缅甸和其他低收入和中等收入国家扩大 HCV 服务的重要组成部分。