Hill Nathan R, Groves Lara, Dickerson Carissa, Ochs Andreas, Pang Dong, Lawton Sarah, Hurst Michael, Pollock Kevin G, Sugrue Daniel M, Tsang Carmen, Arden Chris, Wyn Davies David, Martin Anne Celine, Sandler Belinda, Gordon Jason, Farooqui Usman, Clifton David, Mallen Christian, Rogers Jennifer, Camm Alan John, Cohen Alexander T
Bristol Myers Squibb Pharmaceutical Ltd, Uxbridge, UK.
Health Economics and Outcomes Research Ltd, Cardiff, UK.
Eur Heart J Digit Health. 2022 Mar 23;3(2):195-204. doi: 10.1093/ehjdh/ztac009. eCollection 2022 Jun.
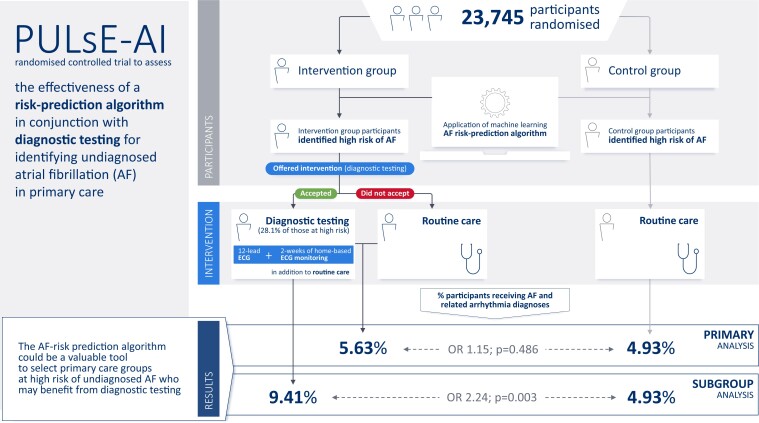
The aim of the PULsE-AI trial was to assess the effectiveness of a machine learning risk-prediction algorithm in conjunction with diagnostic testing for identifying undiagnosed atrial fibrillation (AF) in primary care in England.
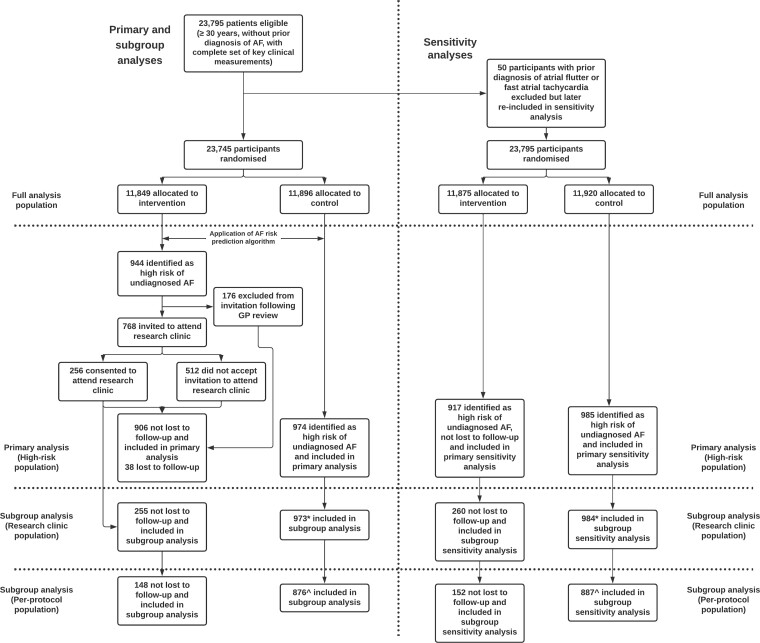
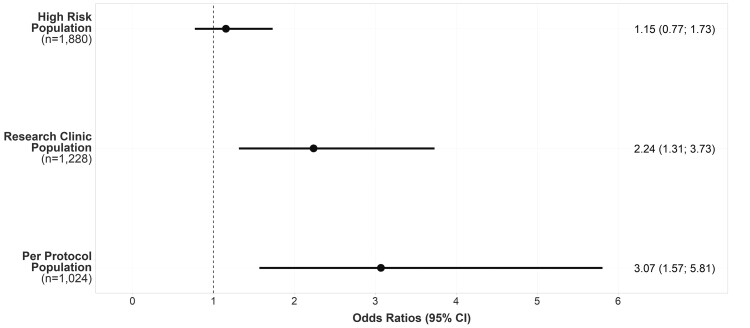
Eligible participants (aged ≥30 years without AF diagnosis; = 23 745) from six general practices in England were randomized into intervention and control arms. Intervention arm participants, identified by the algorithm as high risk of undiagnosed AF ( = 944), were invited for diagnostic testing ( = 256 consented); those who did not accept the invitation, and all control arm participants, were managed routinely. The primary endpoint was the proportion of AF, atrial flutter, and fast atrial tachycardia diagnoses during the trial (June 2019-February 2021) in high-risk participants. Atrial fibrillation and related arrhythmias were diagnosed in 5.63% and 4.93% of high-risk participants in intervention and control arms, respectively {odds ratio (OR) [95% confidence interval (CI)]: 1.15 (0.77-1.73), = 0.486}. Among intervention arm participants who underwent diagnostic testing (28.1%), 9.41% received AF and related arrhythmia diagnoses [vs. 4.93% (control); OR (95% CI): 2.24 (1.31-3.73), = 0.003].
The AF risk-prediction algorithm accurately identified high-risk participants in both arms. While the proportions of AF and related arrhythmia diagnoses were not significantly different between high-risk arms, intervention arm participants who underwent diagnostic testing were twice as likely to receive arrhythmia diagnoses compared with routine care. The algorithm could be a valuable tool to select primary care groups at high risk of undiagnosed AF who may benefit from diagnostic testing.
PULsE-AI试验的目的是评估机器学习风险预测算法结合诊断测试在英格兰初级医疗中识别未诊断心房颤动(AF)的有效性。
来自英格兰六个普通诊所的符合条件的参与者(年龄≥30岁,未诊断为AF;n = 23745)被随机分为干预组和对照组。算法识别为未诊断AF高风险的干预组参与者(n = 944)被邀请进行诊断测试(n = 256同意);未接受邀请的参与者以及所有对照组参与者接受常规管理。主要终点是试验期间(2019年6月至2021年2月)高风险参与者中AF、心房扑动和快速房性心动过速诊断的比例。干预组和对照组中分别有5.63%和4.93%的高风险参与者被诊断为心房颤动和相关心律失常{优势比(OR)[95%置信区间(CI)]:1.15(0.77 - 1.73),P = 0.486}。在接受诊断测试的干预组参与者中(28.1%),9.41%被诊断为AF和相关心律失常[对照组为4.93%;OR(95%CI):2.24(1.31 - 3.73),P = 0.003]。
AF风险预测算法准确识别了两组中的高风险参与者。虽然高风险组之间AF和相关心律失常诊断的比例没有显著差异,但与常规护理相比,接受诊断测试的干预组参与者接受心律失常诊断的可能性是其两倍。该算法可能是一种有价值的工具,用于选择可能从诊断测试中受益的未诊断AF高风险的初级医疗群体。