Stirrup Oliver, Shrotri Madhumita, Adams Natalie L, Krutikov Maria, Nacer-Laidi Hadjer, Azmi Borscha, Palmer Tom, Fuller Christopher, Irwin-Singer Aidan, Baynton Verity, Tut Gokhan, Moss Paul, Hayward Andrew, Copas Andrew, Shallcross Laura
Institute for Global Health, University College London, London, United Kingdom.
UCL Institute of Health Informatics, London, United Kingdom.
Open Forum Infect Dis. 2022 Dec 29;10(1):ofac694. doi: 10.1093/ofid/ofac694. eCollection 2023 Jan.
Successive severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) variants have caused severe disease in long-term care facility (LTCF) residents. Primary vaccination provides strong short-term protection, but data are limited on duration of protection following booster vaccines, particularly against the Omicron variant. We investigated the effectiveness of booster vaccination against infections, hospitalizations, and deaths among LTCF residents and staff in England.
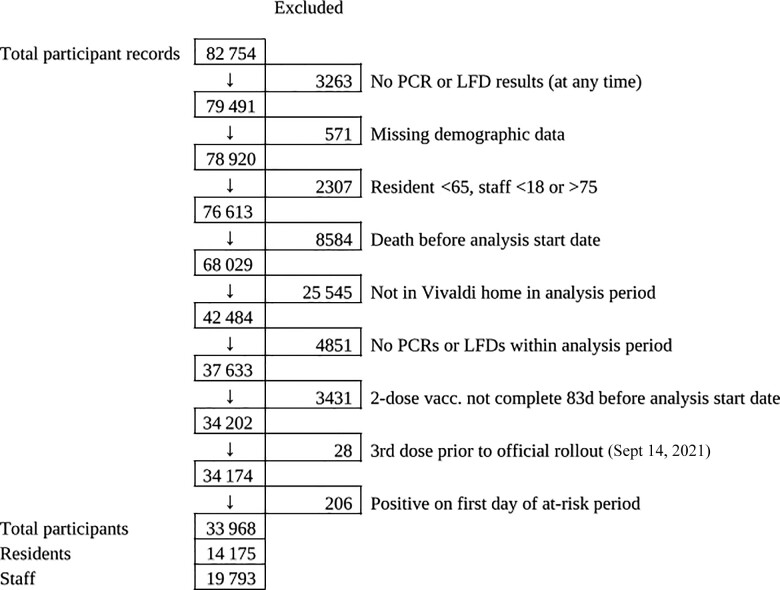
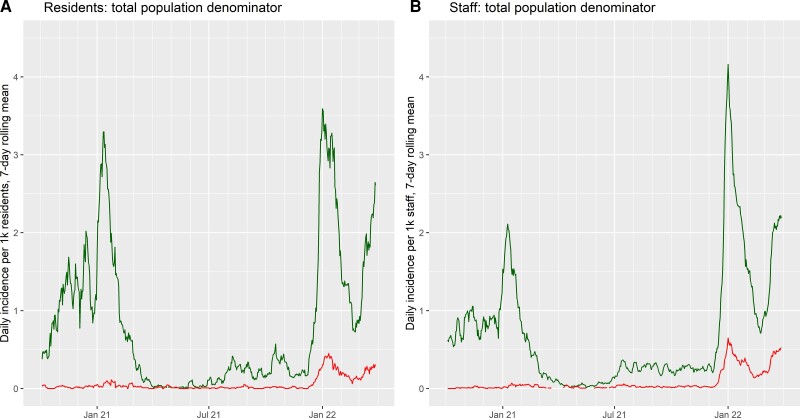
We included residents and staff of LTCFs within the VIVALDI study (ISRCTN 14447421) who underwent routine, asymptomatic testing (December 12, 2021-March 31, 2022). Cox regression was used to estimate relative hazards of SARS-CoV-2 infection, and associated hospitalization and death at 0-13, 14-48, 49-83, 84-111, 112-139, and 140+ days after dose 3 of SARS-CoV-2 vaccination compared with 2 doses (after 84+ days), stratified by previous SARS-CoV-2 infection and adjusting for age, sex, LTCF capacity, and local SARS-CoV-2 incidence.
A total of 14 175 residents and 19 793 staff were included. In residents without prior SARS-CoV-2 infection, infection risk was reduced 0-111 days after the first booster, but no protection was apparent after 112 days. Additional protection following booster vaccination waned but was still present at 140+ days for COVID-associated hospitalization (adjusted hazard ratio [aHR], 0.20; 95% CI, 0.06-0.63) and death (aHR, 0.50; 95% CI, 0.20-1.27). Most residents (64.4%) had received primary course vaccine of AstraZeneca, but this did not impact pre- or postbooster risk. Staff showed a similar pattern of waning booster effectiveness against infection, with few hospitalizations and no deaths.
Our findings suggest that booster vaccination provided sustained protection against severe outcomes following infection with the Omicron variant, but no protection against infection from 4 months onwards. Ongoing surveillance for SARS-CoV-2 in LTCFs is crucial.
严重急性呼吸综合征冠状病毒2(SARS-CoV-2)的连续变异毒株已在长期护理机构(LTCF)居民中引发严重疾病。初次疫苗接种可提供强大的短期保护,但关于加强疫苗接种后的保护持续时间的数据有限,尤其是针对奥密克戎变异毒株。我们调查了加强疫苗接种对英格兰长期护理机构居民和工作人员感染、住院和死亡的有效性。
我们纳入了VIVALDI研究(ISRCTN 14447421)中的长期护理机构居民和工作人员,他们接受了常规无症状检测(2021年12月12日至2022年3月31日)。采用Cox回归估计SARS-CoV-2感染的相对风险,以及在SARS-CoV-2疫苗第3剂接种后0至13天、14至48天、49至83天、84至111天、112至139天和140天及以后与2剂接种(84天及以后)相比的相关住院和死亡风险,按既往SARS-CoV-2感染情况分层,并对年龄、性别、长期护理机构容量和当地SARS-CoV-2发病率进行调整。
共纳入14175名居民和19793名工作人员。在既往无SARS-CoV-2感染的居民中,首次加强疫苗接种后0至111天感染风险降低,但112天后无明显保护作用。加强疫苗接种后的额外保护作用减弱,但在140天及以后仍存在于与新冠相关的住院(调整后风险比[aHR],0.20;95%置信区间[CI],0.06至0.63)和死亡(aHR,0.50;95%CI,0.20至1.27)方面。大多数居民(64.4%)接种了阿斯利康的初级疫苗疗程,但这并未影响加强疫苗接种前后的风险。工作人员在预防感染方面加强疫苗接种效果减弱的模式类似,住院人数很少且无死亡病例。
我们的研究结果表明,加强疫苗接种可对奥密克戎变异毒株感染后的严重后果提供持续保护,但从4个月起对感染无保护作用。对长期护理机构中SARS-CoV-2进行持续监测至关重要。