Department of General Practice, Amsterdam UMC, Location University of Amsterdam, Amsterdam, the Netherlands.
Amsterdam Public Health, Research Programme Quality of Care, and Personalized Medicine, Amsterdam, the Netherlands.
J Natl Cancer Inst. 2023 May 8;115(5):523-529. doi: 10.1093/jnci/djad019.
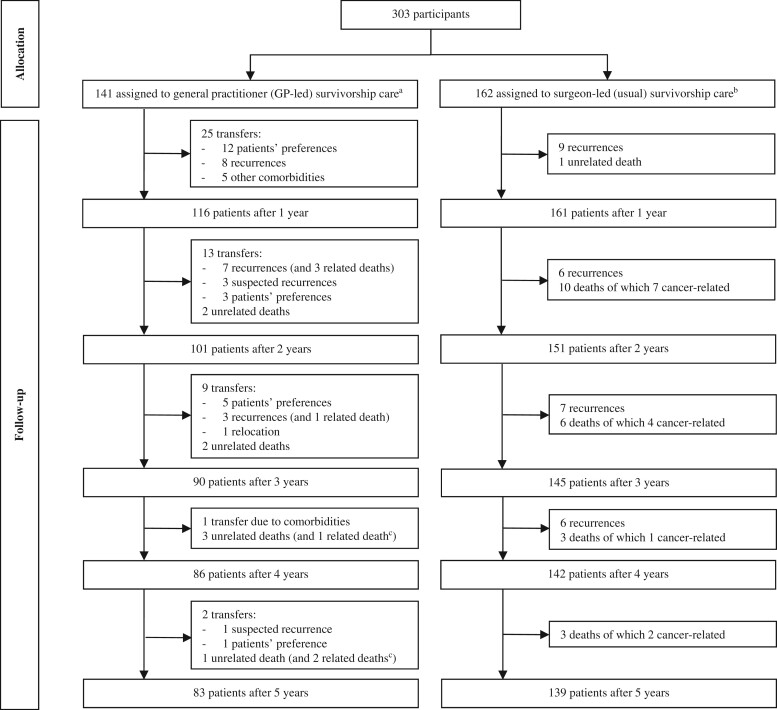
In the I CARE study, colon cancer patients were randomly assigned to receive follow-up care from either a general practitioner (GP) or a surgeon. Here, we address a secondary outcome, namely, detection of recurrences and effect on time to detection of transferring care from surgeon to GP.
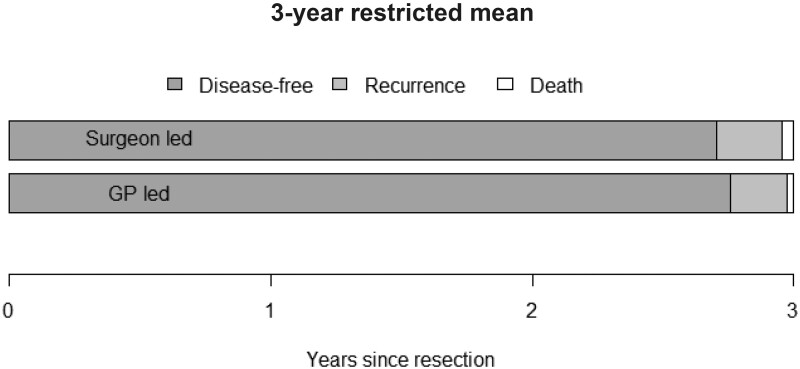
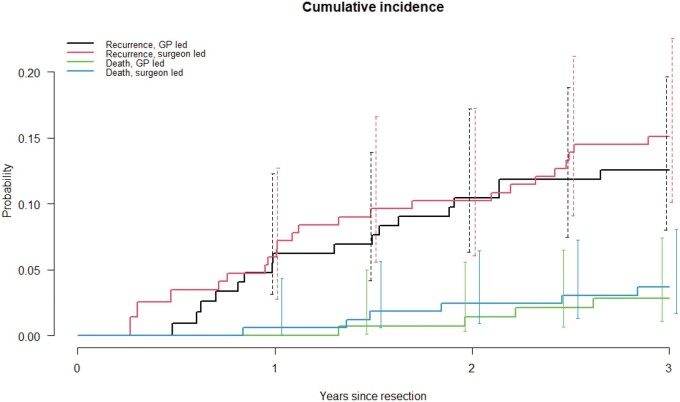
Pattern, stage, and treatment of recurrences were described after 3 years. Time to event was defined as date of surgery, until date of recurrence or last follow-up, with death as competing event. Effects on time to recurrence and death were estimated as hazard ratios (HRs) using Cox regression. Restricted mean survival times were estimated.
Of 303 patients, 141 were randomly assigned to the GP and 162 to the surgeon. Patients were male (67%) with a mean age of 68.0 (8.4) years. During follow-up, 46 recurrences were detected; 18 (13%) in the GP vs 28 (17%) in the surgeon group. Most recurrences were detected via abnormal follow-up tests (74%) and treated with curative intent (59%). Hazard ratio for recurrence was 0.75 (95% confidence interval [CI] = 0.41 to 1.36) in GP vs surgeon group. Patients in the GP group remained in the disease-free state slightly longer (2.76 vs 2.71 years). Of the patients, 38 died during follow-up; 15 (11%) in the GP vs 23 (14%) in the surgeon group. Of these, 21 (55%) deaths were related to colon cancer. There were no differences in overall deaths between the groups (HR = 0.76, 95% CI = 0.39 to 1.46).
Follow-up provided by GPs vs surgeons leads to similar detection of recurrences. Also, no differences in mortality were found.
在 I CARE 研究中,结肠癌患者被随机分配接受全科医生(GP)或外科医生的随访护理。在这里,我们解决了次要结果,即检测复发情况以及将护理从外科医生转移到 GP 对检测时间的影响。
在 3 年后描述了复发的模式、阶段和治疗情况。时间事件定义为手术日期,直至复发日期或最后一次随访日期,以死亡为竞争事件。使用 Cox 回归估计对复发和死亡的时间影响,作为风险比(HRs)。估计限制性平均生存时间。
在 303 名患者中,141 名被随机分配到 GP 组,162 名分配到外科医生组。患者为男性(67%),平均年龄为 68.0(8.4)岁。在随访期间,检测到 46 例复发;GP 组 18 例(13%),外科医生组 28 例(17%)。大多数复发是通过异常随访检查发现的(74%),并采用治愈性治疗(59%)。GP 组的复发风险比为 0.75(95%置信区间[CI] = 0.41 至 1.36)。GP 组的患者保持无疾病状态的时间略长(2.76 年 vs. 2.71 年)。在随访期间,有 38 名患者死亡;GP 组 15 例(11%),外科医生组 23 例(14%)。其中,21 例(55%)死亡与结肠癌有关。两组之间的总死亡率没有差异(HR = 0.76,95% CI = 0.39 至 1.46)。
GP 提供的随访与外科医生提供的随访在检测复发方面效果相当。而且,两组在死亡率方面没有差异。