Department of General Practice, Amsterdam UMC, University of Amsterdam, Amsterdam, The Netherlands.
Department of General Practice, Amsterdam UMC, University of Amsterdam, Amsterdam, The Netherlands
BMJ Open. 2021 Aug 24;11(8):e048985. doi: 10.1136/bmjopen-2021-048985.
The I CARE study (Improving Care After colon canceR treatment in the Netherlands) aims to compare surgeon-led to general practitioner (GP)-led colon cancer survivorship care. Recruitment to the trial took longer than expected. In this descriptive study, recruitment is critically reviewed.
Patients were recruited from eight Dutch medical centres.
Patients treated with curative intent for stages I-III colon cancer. Target patient sample size was calculated at 300.
Patients were randomised to surgeon-led (usual) versus GP-led care, with or without access to an eHealth application (Oncokompas).
Baseline characteristics of (non-)participants, reasons for non-participation and strategies to improve recruitment were reviewed.
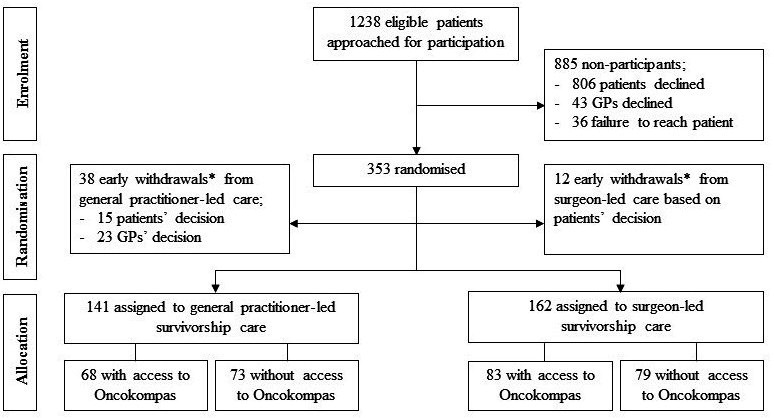
Out of 1238 eligible patients, 353 patients were included. Of these, 50 patients dropped out shortly after randomisation and before start of the intervention, resulting in a participation rate of 25%. Participants were on average slightly younger (68.1 years vs 69.3 years) and more often male (67% vs 50%) in comparison to non-participants. A total of 806 patients declined participation for reasons most often relating to research (57%), including the wish to remain in specialist care (31%) and too much effort to participate (12%). Some patients mentioned health (9%) and confrontation with the disease (5%) as a reason. In 43 cases, GPs declined participation, often related to the study objective, need for financial compensation and time restraints. The generally low participation rate led to concerns about reaching the target sample size. Methods to overcome recruitment challenges included changes to the original recruitment procedure and the addition of new study centres.
Challenges were faced in the recruitment to a randomised trial on GP-led colon cancer survivorship care. Research on the transition of care requires sufficient time, funding and support base among patients and healthcare professionals. These findings will help inform researchers and policy-makers on the development of future practices.
NTR4860.
I CARE 研究(改善荷兰结肠癌治疗后的护理)旨在比较外科医生主导与全科医生(GP)主导的结肠癌生存护理。该试验的招募时间比预期的要长。在这项描述性研究中,对招募工作进行了严格审查。
患者从荷兰的 8 个医疗中心招募。
接受根治性治疗的 I-III 期结肠癌患者。目标患者样本量预计为 300 例。
患者被随机分配到外科医生主导(常规)与 GP 主导的护理,可选择或不选择电子健康应用程序(Oncokompas)。
回顾非参与者的基线特征、不参与的原因以及改进招募的策略。
在 1238 名符合条件的患者中,有 353 名患者入选。其中,50 名患者在随机分组后和干预开始前不久退出,参与率为 25%。与非参与者相比,参与者平均年龄稍小(68.1 岁比 69.3 岁),且男性比例更高(67%比 50%)。共有 806 名患者因各种原因拒绝参与,最常见的原因与研究有关(57%),包括希望继续接受专科治疗(31%)和参与的努力太大(12%)。一些患者提到健康(9%)和与疾病对抗(5%)是原因。在 43 例情况下,GP 拒绝参与,通常与研究目的、经济补偿需求和时间限制有关。总的来说,参与率较低,这引起了对达到目标样本量的担忧。克服招募挑战的方法包括改变最初的招募程序和增加新的研究中心。
在随机试验中,GP 主导的结肠癌生存护理的招募面临挑战。护理的过渡研究需要患者和医疗保健专业人员有足够的时间、资金和支持基础。这些发现将有助于为研究人员和政策制定者提供未来实践的信息。
NTR4860。