Department of General Practice, Amsterdam UMC, University of Amsterdam, Meibergdreef 9, 1105 AZ, Amsterdam, the Netherlands.
Amsterdam Public Health Research Institute, Amsterdam, the Netherlands.
J Cancer Surviv. 2024 Aug;18(4):1393-1402. doi: 10.1007/s11764-023-01383-4. Epub 2023 Apr 25.
The aim of this study is to assess cost-effectiveness of general practitioner (GP) versus surgeon-led colon cancer survivorship care from a societal perspective.
We performed an economic evaluation alongside the I CARE study, which included 303 cancer patients (stages I-III) who were randomised to survivorship care by a GP or surgeon. Questionnaires were administered at baseline, 3-, 6-, 12-, 24- and 36-months. Costs included healthcare costs (measured by iMTA MCQ) and lost productivity costs (SF-HLQ). Disease-specific quality of life (QoL) was measured using EORTC QLQ-C30 summary score and general QoL using EQ-5D-3L quality-adjusted life years (QALYs). Missing data were imputed. Incremental cost-effectiveness ratios (ICERs) were calculated to relate costs to effects on QoL. Statistical uncertainty was estimated using bootstrapping.
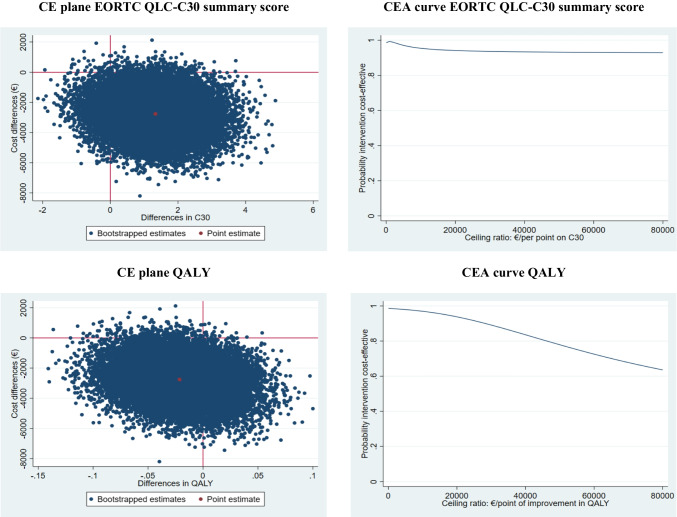
Total societal costs of GP-led care were significantly lower compared to surgeon-led care (mean difference of - €3895; 95% CI - €6113; - €1712). Lost productivity was the main contributor to the difference in societal costs (- €3305; 95% CI - €5028; - €1739). The difference in QLQ-C30 summary score over time between groups was 1.33 (95% CI - 0.049; 3.15). The ICER for QLQ-C30 was - 2073, indicating that GP-led care is dominant over surgeon-led care. The difference in QALYs was - 0.021 (95% CI - 0.083; 0.040) resulting in an ICER of 129,164.
GP-led care is likely to be cost-effective for disease-specific QoL, but not for general QoL.
With a growing number of cancer survivors, GP-led survivorship care could help to alleviate some of the burden on more expensive secondary healthcare services.
本研究旨在从社会角度评估全科医生(GP)与外科医生主导的结肠癌生存护理的成本效益。
我们在 I CARE 研究中进行了一项经济评估,该研究纳入了 303 名癌症患者(I-III 期),他们被随机分配接受 GP 或外科医生的生存护理。在基线、3、6、12、24 和 36 个月时进行问卷调查。成本包括医疗保健成本(通过 iMTA MCQ 衡量)和生产力损失成本(SF-HLQ)。使用 EORTC QLQ-C30 综合评分和 EQ-5D-3L 质量调整生命年(QALYs)来衡量特定于疾病的生活质量(QoL)。缺失数据采用插补法处理。计算增量成本效益比(ICER)以将成本与 QoL 效果相关联。使用自举法估计统计不确定性。
与外科医生主导的护理相比,GP 主导的护理的总社会成本显著降低(平均差异为-€3895;95%CI-€6113;-€1712)。生产力损失是社会成本差异的主要原因(-€3305;95%CI-€5028;-€1739)。两组之间的 QLQ-C30 综合评分随时间的差异为 1.33(95%CI-€0.049;3.15)。QLQ-C30 的 ICER 为-2073,表明 GP 主导的护理优于外科医生主导的护理。QALYs 的差异为-0.021(95%CI-€0.083;0.040),导致 ICER 为 129164。
GP 主导的护理可能在疾病特异性 QoL 方面具有成本效益,但在一般 QoL 方面则不然。
随着癌症幸存者人数的增加,GP 主导的生存护理可能有助于减轻更昂贵的二级医疗保健服务的一些负担。