Department of Laboratory Medicine and Pathology, University of Washington School of Medicine, Seattle, WA, USA.
Division of Critical Care Medicine, Department of Anesthesiology and Pain Medicine, University of Washington, Seattle, WA, USA.
Lancet Infect Dis. 2023 Jun;23(6):740-750. doi: 10.1016/S1473-3099(22)00879-9. Epub 2023 Jan 30.
Shigella spp have been associated with community-wide outbreaks in urban settings. We analysed a sustained shigellosis outbreak in Seattle, WA, USA, to understand its origins and mechanisms of antimicrobial resistance, define ongoing transmission patterns, and optimise strategies for treatment and infection control.
We did a retrospective study of all Shigella isolates identified from stool samples at the clinical laboratories at Harborview Medical Center and University of Washington Medical Center (Seattle, WA, USA) from May 1, 2017, to Feb 28, 2022. We characterised isolates by species identification, phenotypic susceptibility testing, and whole-genome sequencing. Demographic characteristics and clinical outcomes of the patients were retrospectively examined.
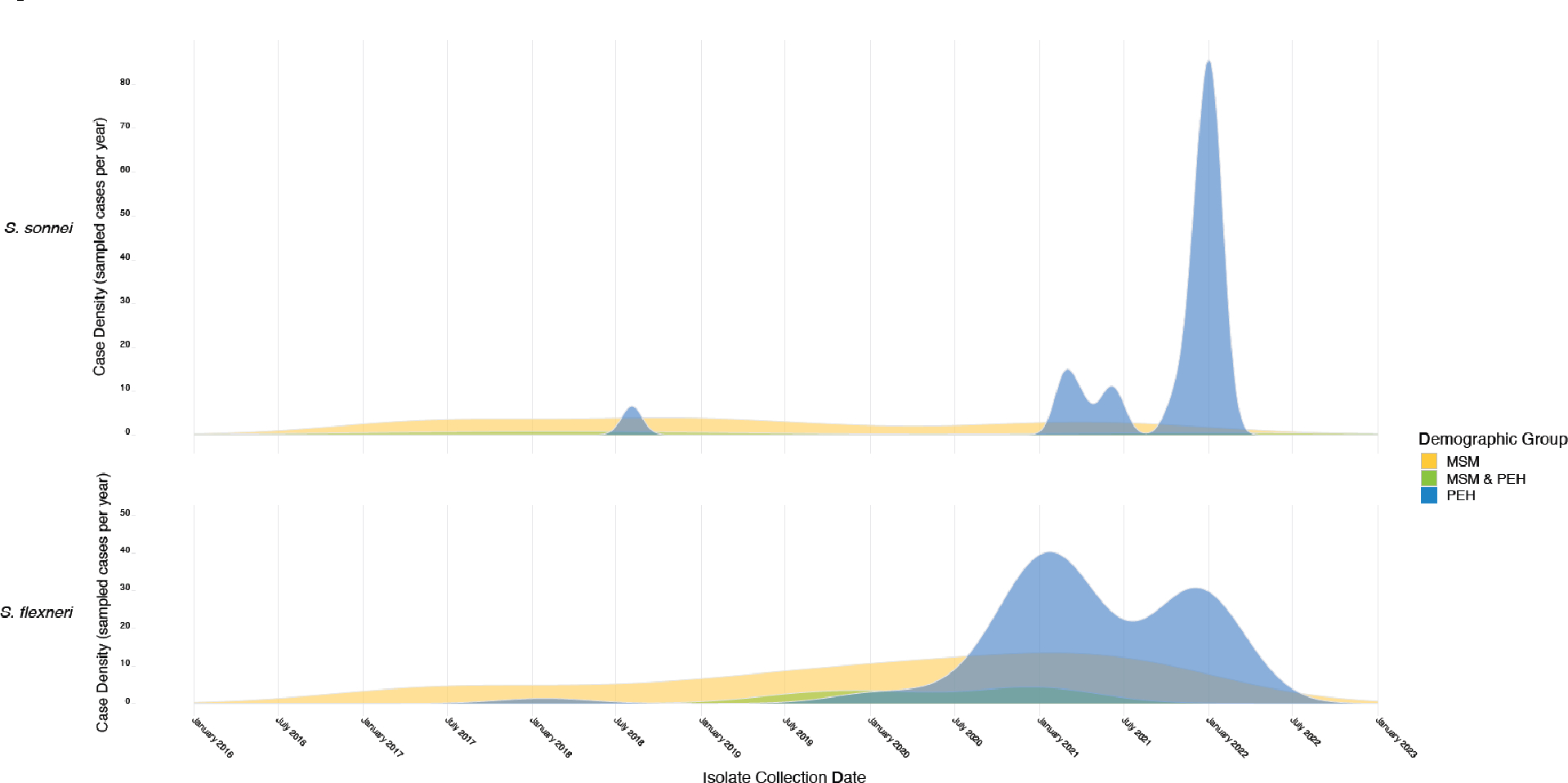
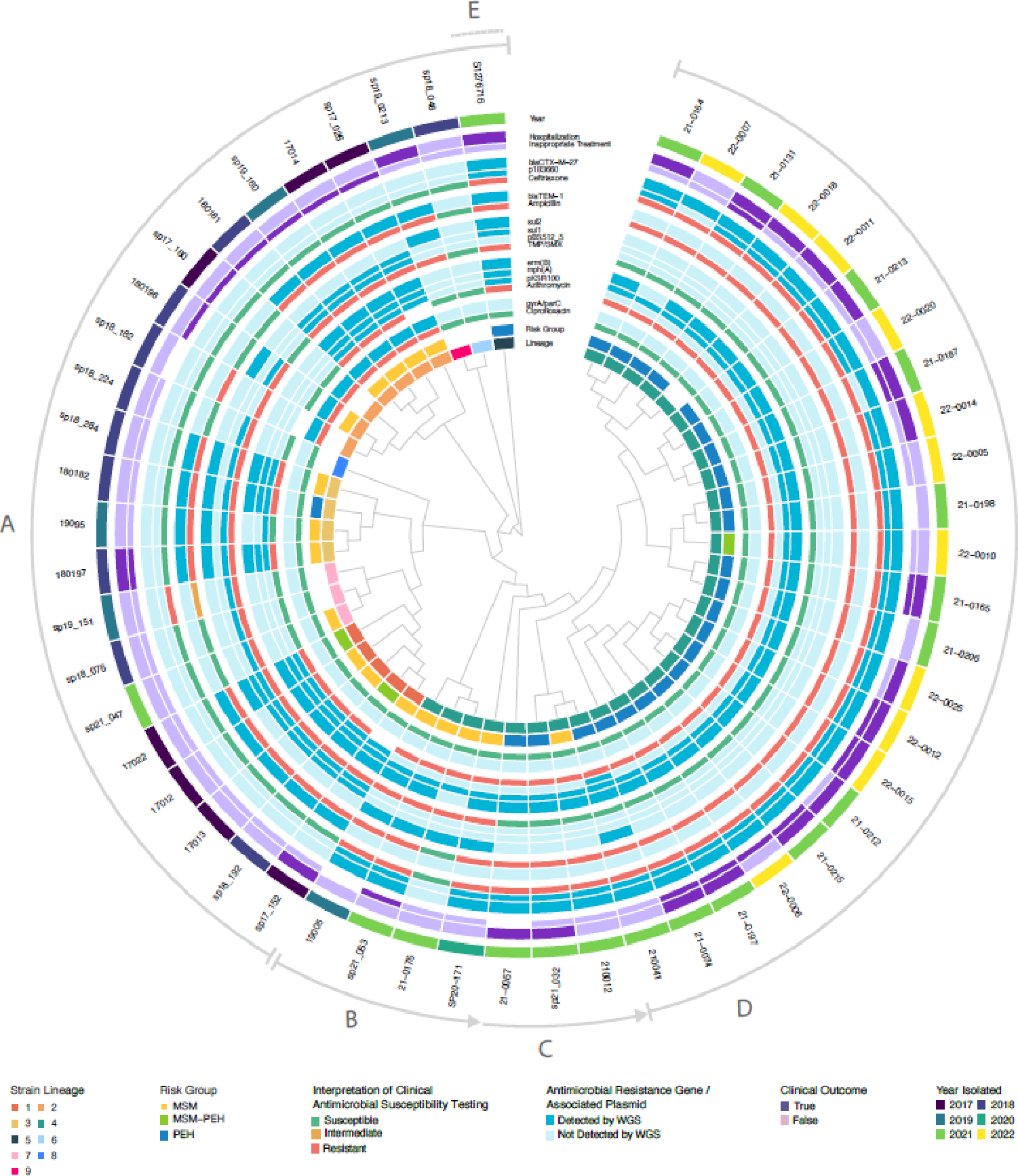
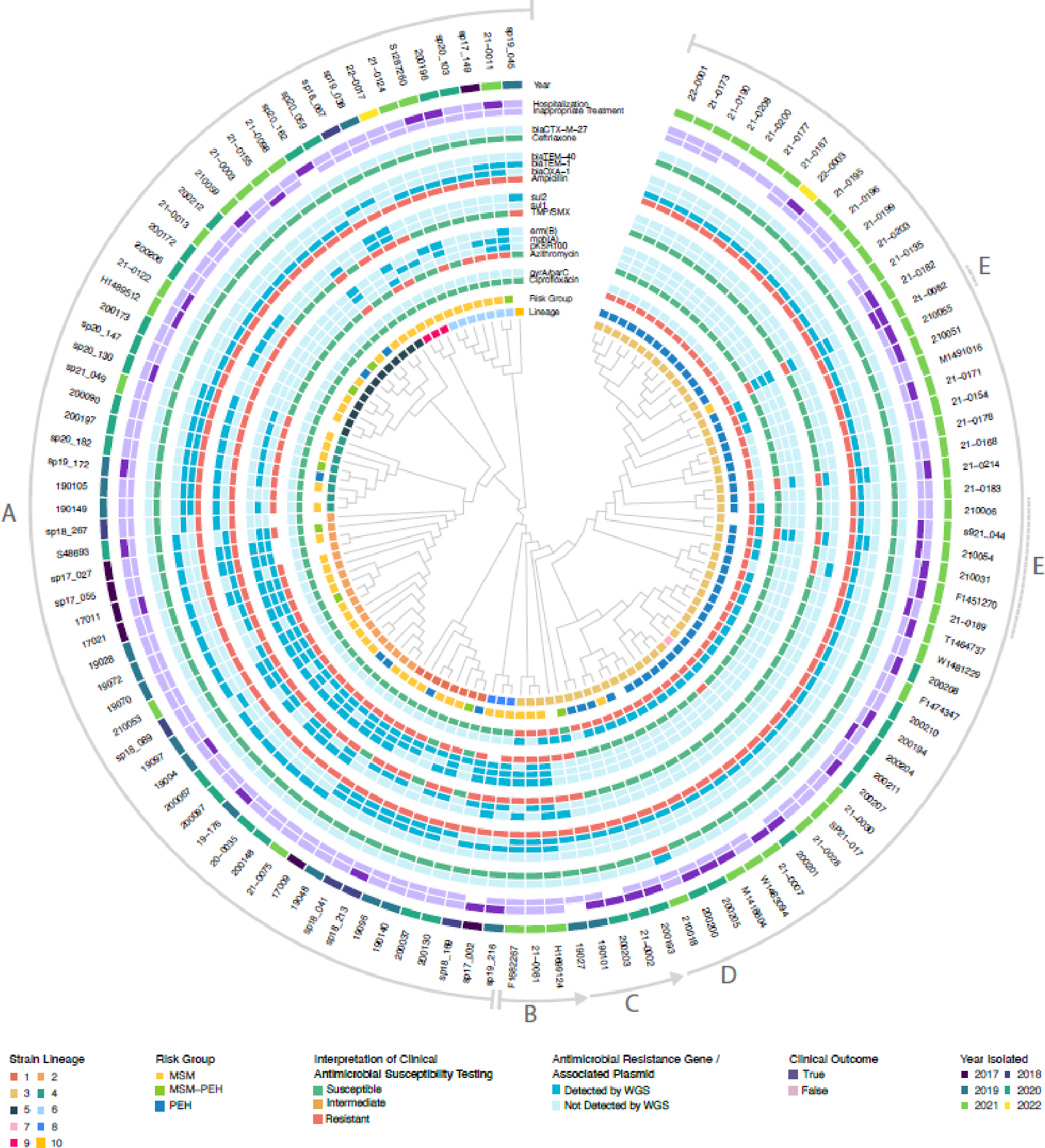
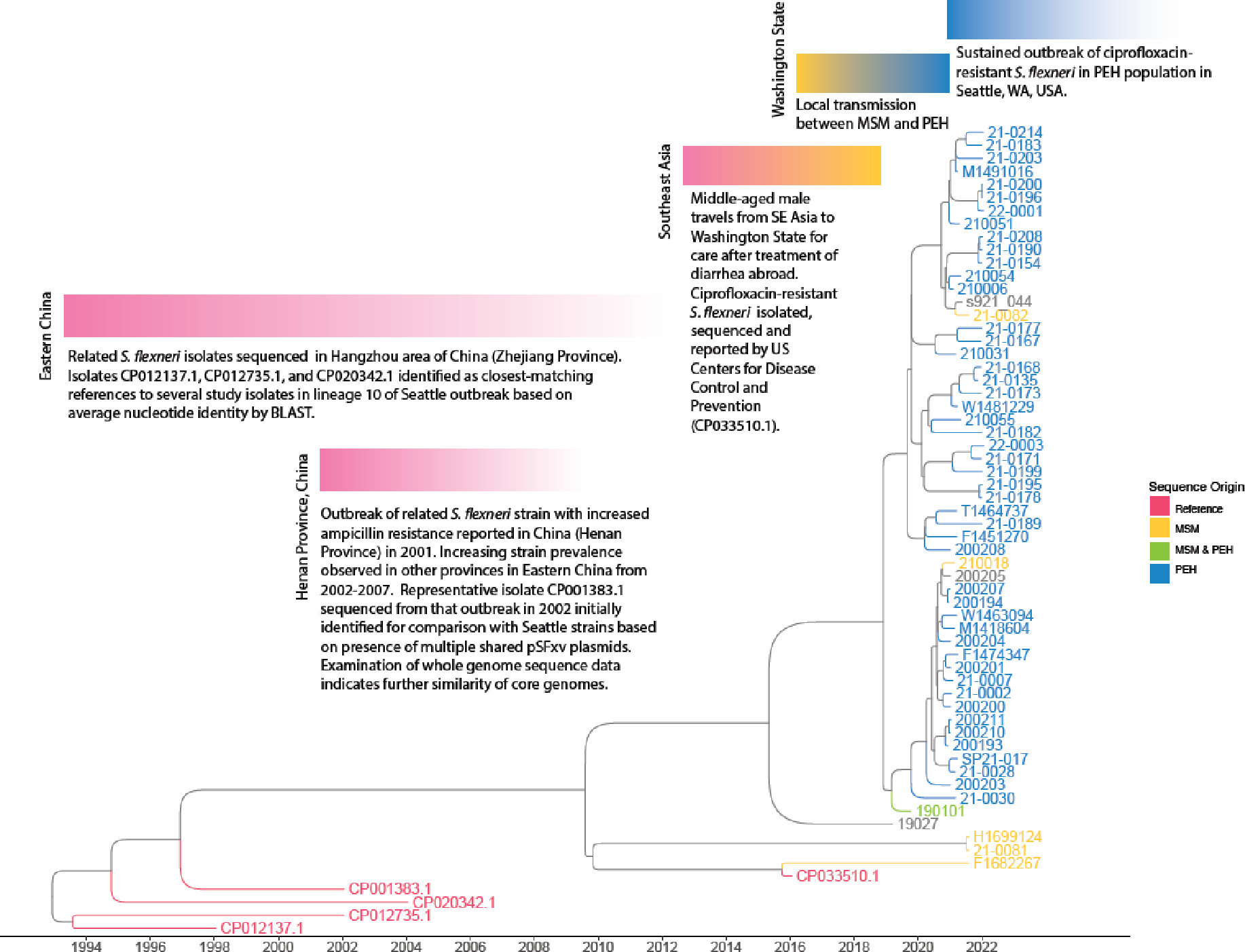
171 cases of shigellosis were included. 78 (46%) patients were men who have sex with men (MSM), and 88 (52%) were people experiencing homelessness (PEH). Although 84 (51%) isolates were multidrug resistant, 100 (70%) of 143 patients with data on antimicrobial therapy received appropriate empirical therapy. Phylogenomic analysis identified sequential outbreaks of multiple distinct lineages of Shigella flexneri and Shigella sonnei. Discrete clonal lineages (ten in S flexneri and nine in S sonnei) and resistance traits were responsible for infection in different at-risk populations (ie, MSM, PEH), enabling development of effective guidelines for empirical treatment. The most prevalent lineage in Seattle was probably introduced to Washington State via international travel, with subsequent domestic transmission between at-risk groups.
An outbreak in Seattle was driven by parallel emergence of multidrug-resistant strains involving international transmission networks and domestic transmission between at-risk populations. Genomic analysis elucidated not only outbreak origin, but directed optimal approaches to testing, treatment, and public health response. Rapid diagnostics combined with detailed knowledge of local epidemiology can enable high rates of appropriate empirical therapy even in multidrug-resistant infection.
None.
志贺氏菌与城市环境中的社区范围暴发有关。我们分析了美国华盛顿州西雅图市持续的志贺氏菌病暴发,以了解其起源和抗微生物药物耐药机制,确定正在进行的传播模式,并优化治疗和感染控制策略。
我们对 2017 年 5 月 1 日至 2022 年 2 月 28 日期间,Harborview 医疗中心和华盛顿大学医疗中心(西雅图,华盛顿州,美国)临床实验室从粪便样本中鉴定出的所有志贺氏菌分离株进行了回顾性研究。我们通过物种鉴定、表型药敏试验和全基因组测序对分离株进行了特征描述。回顾性检查了患者的人口统计学特征和临床结局。
共纳入 171 例志贺氏菌病病例。78 例(46%)患者为男男性行为者(MSM),88 例(52%)为无家可归者(PEH)。虽然 84 例(51%)分离株为多药耐药株,但 143 例有抗菌治疗数据的患者中,有 100 例(70%)接受了适当的经验性治疗。系统发育基因组分析鉴定出多重耐药的福氏志贺菌和宋内志贺菌的多个不同谱系的连续暴发。不同的克隆谱系(福氏志贺菌 10 个,宋内志贺菌 9 个)和耐药特征导致不同高危人群(即 MSM、PEH)发生感染,为经验性治疗制定了有效的指南。西雅图最常见的谱系可能是通过国际旅行传入华盛顿州的,随后在高危人群之间发生了国内传播。
西雅图的暴发是由涉及国际传播网络和高危人群之间国内传播的多重耐药菌株的平行出现驱动的。基因组分析不仅阐明了暴发的起源,而且为检测、治疗和公共卫生应对提供了最佳方法。快速诊断加上对当地流行病学的详细了解,可以实现高比例的适当经验性治疗,即使在多重耐药感染中也是如此。
无。