Heart Rhythm Management Centre, Postgraduate Program in Cardiac Electrophysiology and Pacing, Universitair Ziekenhuis Brussel-Vrije Universiteit Brussel, European Reference Networks Guard-Heart, Laarbeeklaan 101, 1090, Brussels, Belgium.
Cardiac Surgery Department, Universitair Ziekenhuis Brussel-Vrije Universiteit Brussel, Laarbeeklaan 101, 1090, Brussels, Belgium.
Europace. 2023 Mar 30;25(3):896-904. doi: 10.1093/europace/euad017.
The multielectrode radiofrequency balloon catheter (RFB) has been developed to achieve safe and effective pulmonary vein isolation (PVI) for atrial fibrillation (AF) ablation. This single-centre study aimed to evaluate the midterm clinical outcome and predictors of single-shot PVI with the novel RFB.
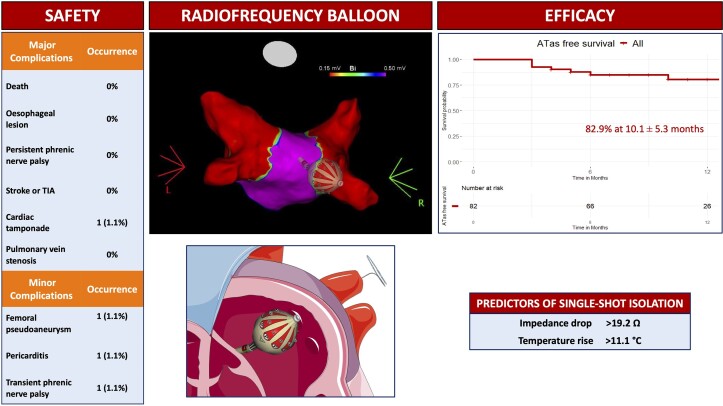
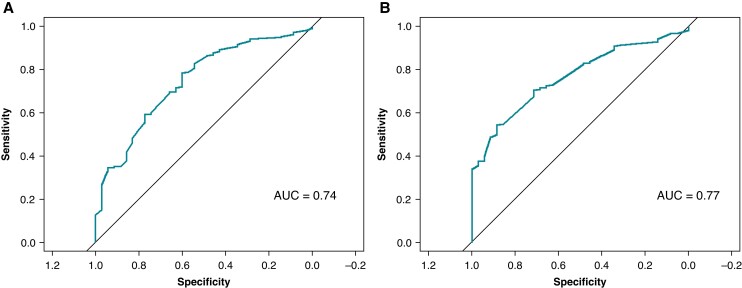
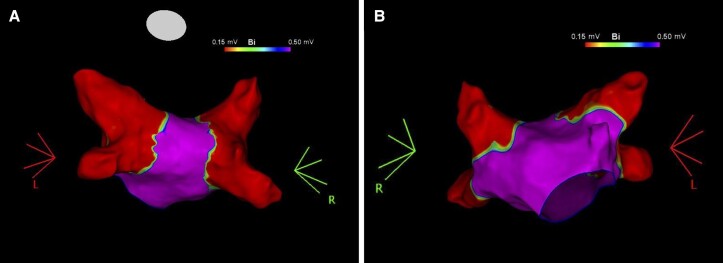
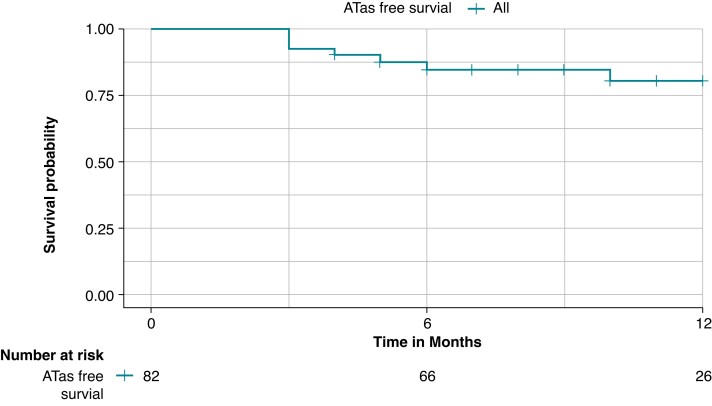
All consecutive patients with symptomatic paroxysmal or persistent AF undergoing first-time PVI with the RFB were prospectively included. Clinical and procedural parameters were systematically collected. The primary safety endpoint was defined as any major periprocedural complications. The primary efficacy endpoint consisted of freedom from any atrial tachyarrhythmias (ATas) lasting >30 s during the follow-up after a 3-month blanking period. Persistent single-shot PVI was defined as PVI achieved with a single RFB application without acute reconnection. A total of 104 consecutive patients (mean age 64.3 ± 11.4 years, 56.7% males) were included. 15 patients (14.4%) presented with persistent AF. The procedure time was 59.0 min with a dwell time of 20.0 min. One major complication occurred in one patient. At a mean follow-up of 10.1 ± 5.3 months, freedom from ATas was 82.9%. ATas occurred in 14 patients, 11/69 patients (15.9%) with paroxysmal AF and 3/13 (23.1%) with persistent AF. The best cut-offs to predict persistent single-shot PVI were impedance drop >19.2 Ω [area under the receiver operator characteristic curve (AUC) 0.74] and temperature rise >11.1° C (AUC 0.77).
In a large cohort of patients undergoing PVI with the RFB, the complication rate was 1%. At a mid-term follow-up of 10.1 ± 5.3 months, freedom from ATas was 82.9%. Specific cut-offs of impedance drop and temperature rise may be useful to predict persistent single-shot isolation.
多电极射频球囊导管(RFB)的开发旨在实现安全有效的肺静脉隔离(PVI),用于房颤(AF)消融。本单中心研究旨在评估新型 RFB 单次 PVI 的中期临床结果和预测因素。
所有连续因症状性阵发性或持续性 AF 而接受 RFB 首次 PVI 的患者均前瞻性纳入本研究。系统收集临床和程序参数。主要安全性终点定义为任何围手术期重大并发症。主要疗效终点包括在 3 个月空白期后随访期间,无任何持续时间>30s 的房性快速性心律失常(ATas)。持续性单次 PVI 定义为单次 RFB 应用即可实现 PVI,且无急性再连接。共纳入 104 例连续患者(平均年龄 64.3±11.4 岁,56.7%为男性)。15 例(14.4%)患者持续性 AF。手术时间为 59.0 分钟,驻留时间为 20.0 分钟。1 例患者发生 1 例重大并发症。平均随访 10.1±5.3 个月时,无 ATas 的比例为 82.9%。14 例患者发生 ATas,69 例阵发性 AF 患者中 11 例(15.9%),13 例持续性 AF 患者中 3 例(23.1%)。预测持续性单次 PVI 的最佳截断值为阻抗下降>19.2 Ω[受试者工作特征曲线下面积(AUC)为 0.74]和温度升高>11.1°C(AUC 为 0.77)。
在接受 RFB 行 PVI 的大患者队列中,并发症发生率为 1%。在 10.1±5.3 个月的中期随访中,无 ATas 的比例为 82.9%。阻抗下降和温度升高的特定截断值可能有助于预测持续性单次隔离。