Morenz Anna, Perkins James, Dick André, Young Bessie, Ng Yue-Harn
Department of Medicine, University of Washington, Seattle, WA.
Clinical and Bio-Analytics Transplant Laboratory (CBATL), Department of Surgery, University of Washington, Seattle, WA.
Transplant Direct. 2023 Jan 26;9(2):e1442. doi: 10.1097/TXD.0000000000001442. eCollection 2023 Feb.
Insurance type, a marker of socioeconomic status, has been associated with poor access to kidney transplant (KT) and worse KT outcomes before the implementation of the Affordable Care Act (ACA) and the revised Kidney Allocation System (KAS). In this study, we assessed if insurance type remained a risk marker for worse waitlist and transplant outcomes after ACA and KAS.
Using Scientific Registry of Transplant Recipients data, we assessed insurance type of waitlisted candidates pre- (2008-2014) versus post- (2014-2021) KAS/ACA using chi-square tests. Next, we performed a competing risk analysis to study the effect of private versus public (Medicare, Medicaid, or government-sponsored) insurance on waitlist outcomes and a Cox survival analysis to study posttransplant outcomes while controlling for candidate, and recipient and donor variables, respectively.
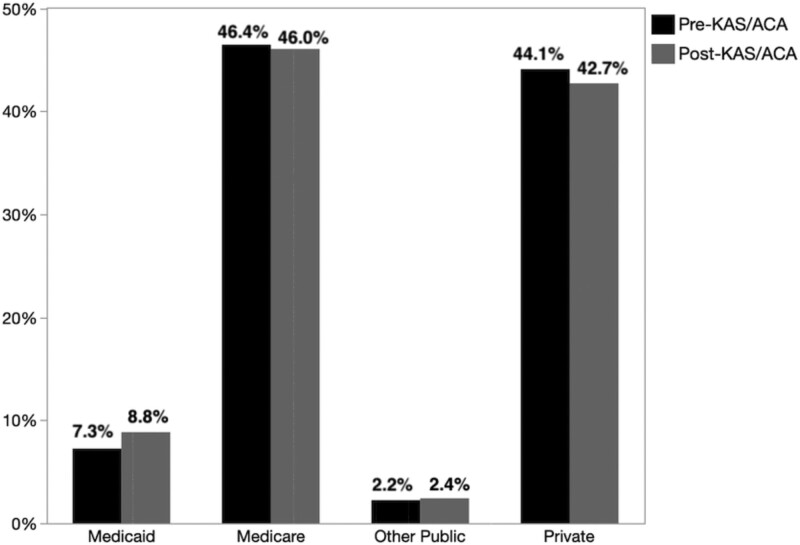
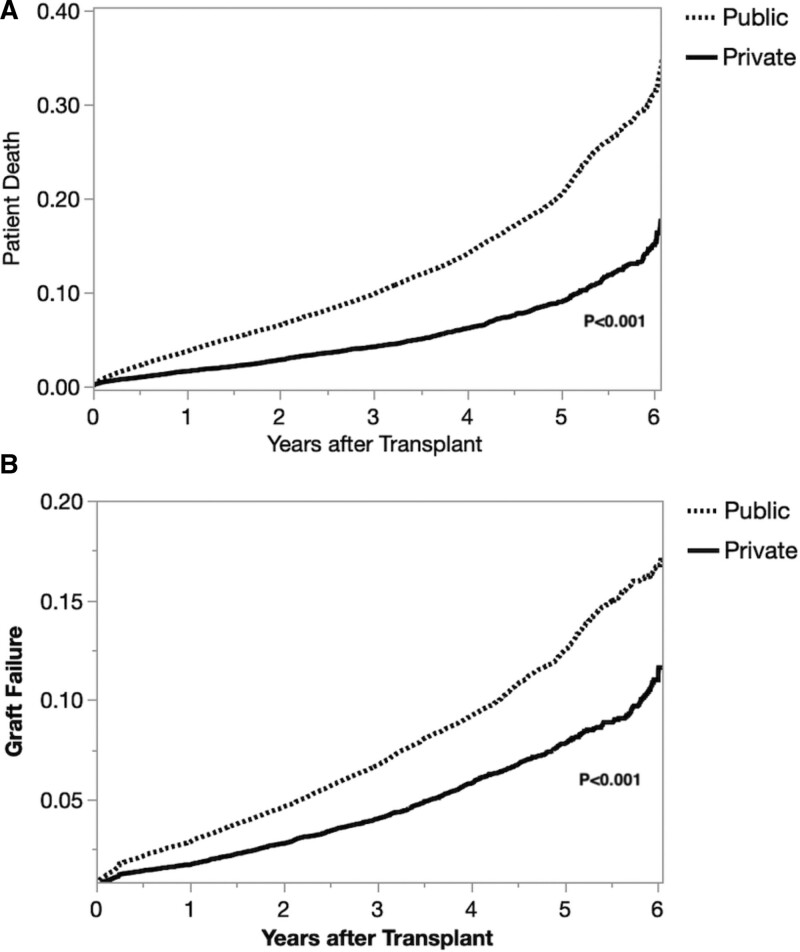
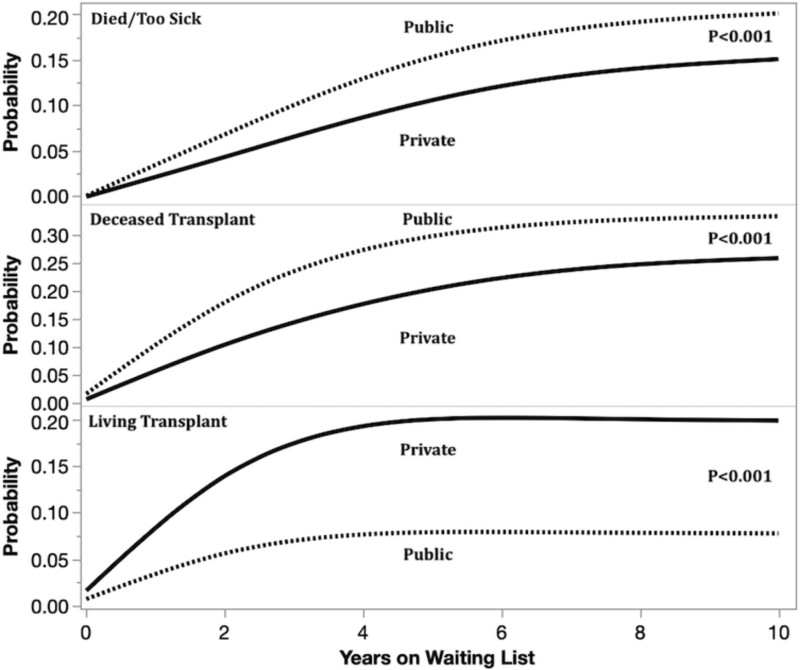
The proportion of overall KT candidates insured by Medicaid increased from pre-KAS/ACA to post-KAS/ACA (from 12 667 [7.3%] to 21 768 [8.8%], < 0.0001). However, KT candidates with public insurance were more likely to have died or become too sick for KT (subdistribution hazard ratio [SHR] = 1.33, confidence interval [CI], 1.30-1.36) or to receive a deceased donor KT (SHR = 1.57, CI, 1.54-1.60) but less likely to receive a living donor KT (SHR = 0.87, CI, 0.85-0.89). Post-KT, KT recipients with public insurance had greater risk of mortality (relative risks = 1.22, CI, 1.15-1.31) and allograft failure (relative risks = 1.10, CI, 1.03-1.29).
Although the implementation of ACA marginally increased the proportion of waitlisted candidates with Medicaid, publicly insured KT candidates remained at greater risk of being removed from the waitlist, had lower probability of living donor kidney transplantation, and had greater probability of dying post-KT and allograft failure. Concerted efforts to address factors contributing to these inequities in future studies are needed, with the goal of achieving equity in KT for all.
保险类型作为社会经济地位的一个指标,在《平价医疗法案》(ACA)和修订后的肾脏分配系统(KAS)实施之前,就与肾脏移植(KT)机会少及KT结果较差有关。在本研究中,我们评估了在ACA和KAS实施后,保险类型是否仍然是等待名单和移植结果较差的风险指标。
利用移植受者科学登记处的数据,我们使用卡方检验评估了KAS/ACA实施前(2008 - 2014年)与实施后(2014 - 2021年)等待名单上候选人的保险类型。接下来,我们进行了竞争风险分析,以研究私人保险与公共保险(医疗保险、医疗补助或政府资助保险)对等待名单结果的影响,并进行了Cox生存分析,以研究移植后的结果,同时分别控制候选人、受者和供者变量。
由医疗补助承保的总体KT候选人比例从KAS/ACA实施前到实施后有所增加(从12667人[7.3%]增至21768人[8.8%],<0.0001)。然而,有公共保险的KT候选人更有可能死亡或因病情过重而无法进行KT(亚分布风险比[SHR]=1.33,置信区间[CI],1.30 - 1.36)或接受 deceased donor KT(SHR = 1.57,CI,1.54 - 1.60),但接受活体供者KT的可能性较小(SHR = 0.87,CI,0.85 - 0.89)。KT后,有公共保险的KT受者死亡风险(相对风险=1.22,CI,1.15 - 1.31)和移植肾失功风险(相对风险=1.10,CI,1.03 - 1.29)更高。
尽管ACA的实施使等待名单上有医疗补助的候选人比例略有增加,但有公共保险的KT候选人从等待名单上被移除的风险仍然更高,活体供者肾移植的可能性更低,KT后死亡和移植肾失功的可能性更大。未来研究需要共同努力解决导致这些不平等的因素,目标是实现所有人在KT方面的公平。