Pharmaceutical Care Department, King Abdulaziz Medical City (KAMC)-Ministry of National Guard Health Affairs (MNGHA), Riyadh, Saudi Arabia.
College of Pharmacy, King Saud bin Abdulaziz University for Health Sciences, PO Box 22490, Riyadh, 11426, Saudi Arabia.
BMC Infect Dis. 2023 Feb 6;23(1):75. doi: 10.1186/s12879-023-08010-8.
Previous studies have shown that non-critically ill COVID-19 patients co-infected with other respiratory viruses have poor clinical outcomes. However, limited studies focused on this co-infections in critically ill patients. This study aims to evaluate the clinical outcomes of critically ill patients infected with COVID-19 and co-infected by other respiratory viruses.
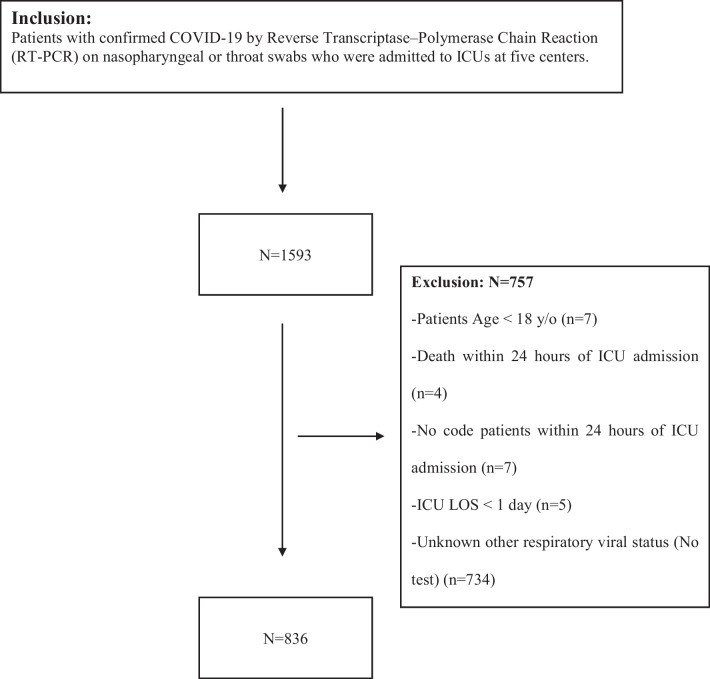
A multicenter retrospective cohort study was conducted for all adult patients with COVID-19 who were hospitalized in the ICUs between March, 2020 and July, 2021. Eligible patients were sub-categorized into two groups based on simultaneous co-infection with other respiratory viruses throughout their ICU stay. Influenza A or B, Human Adenovirus (AdV), Human Coronavirus (i.e., 229E, HKU1, NL63, or OC43), Human Metapneumovirus, Human Rhinovirus/Enterovirus, Middle East Respiratory Syndrome Coronavirus (MERS-CoV), Parainfluenza virus, and Respiratory Syncytial Virus (RSV) were among the respiratory viral infections screened. Patients were followed until discharge from the hospital or in-hospital death.
A total of 836 patients were included in the final analysis. Eleven patients (1.3%) were infected concomitantly with other respiratory viruses. Rhinovirus/Enterovirus (38.5%) was the most commonly reported co-infection. No difference was observed between the two groups regarding the 30-day mortality (HR 0.39, 95% CI 0.13, 1.20; p = 0.10). The in-hospital mortality was significantly lower among co-infected patients with other respiratory viruses compared with patients who were infected with COVID-19 alone (HR 0.32 95% CI 0.10, 0.97; p = 0.04). Patients concomitantly infected with other respiratory viruses had longer median mechanical ventilation (MV) duration and hospital length of stay (LOS).
Critically ill patients with COVID-19 who were concomitantly infected with other respiratory viruses had comparable 30-day mortality to those not concomitantly infected. Further proactive testing and care may be required in the case of co-infection with respiratory viruses and COVID-19. The results of our study need to be confirmed by larger studies.
先前的研究表明,合并其他呼吸道病毒感染的非重症 COVID-19 患者临床结局较差。然而,针对重症患者合并感染的研究较少。本研究旨在评估合并其他呼吸道病毒感染的重症 COVID-19 患者的临床结局。
对 2020 年 3 月至 2021 年 7 月期间入住 ICU 的所有成年 COVID-19 患者进行了一项多中心回顾性队列研究。根据患者 ICU 期间是否同时合并其他呼吸道病毒感染,将符合条件的患者分为两组。筛选的呼吸道病毒感染包括甲型或乙型流感病毒、人腺病毒(AdV)、人类冠状病毒(即 229E、HKU1、NL63 或 OC43)、人偏肺病毒、人类鼻病毒/肠道病毒、中东呼吸综合征冠状病毒(MERS-CoV)、副流感病毒和呼吸道合胞病毒(RSV)。患者随访至出院或院内死亡。
最终纳入 836 例患者进行分析。11 例(1.3%)患者同时合并其他呼吸道病毒感染。鼻病毒/肠道病毒(38.5%)是最常见的合并感染。两组间 30 天死亡率无差异(HR 0.39,95%CI 0.13,1.20;p=0.10)。合并其他呼吸道病毒感染的患者院内死亡率显著低于单纯 COVID-19 感染患者(HR 0.32,95%CI 0.10,0.97;p=0.04)。合并其他呼吸道病毒感染的患者机械通气(MV)时间和住院时间中位数均较长。
合并其他呼吸道病毒感染的重症 COVID-19 患者 30 天死亡率与未合并感染的患者相当。对于合并呼吸道病毒和 COVID-19 感染的患者,可能需要进行更积极的检测和治疗。本研究结果需要更大规模的研究加以证实。