From the Department of Surgery (A.L.C., E.E.M., A.S., T.R.S., M.D., M.F., A.G., M.J.C., C.C.S.), School of Medicine, University of Colorado; Ernest E Moore Shock Trauma Center at Denver Health (E.E.M.), Denver; Department of Health Systems, Management and Policy (A.S.), School of Public Health, University of Colorado Denver, Aurora, Colorado; Faculdade Israelita de Ciências da Saúde Albert Einstein (P.H.C.), Hospital Israelita Albert Einstein, São Paulo, Brazil; University of Colorado School of Medicine Proteomics Core Facility (K.H.) and Department of Pediatrics (C.C.S.), School of Medicine, University of Colorado Denver, Aurora; Vitalant Research Division (C.C.S.), Denver, Colorado; and Department of Vascular Surgery (C.J.F.), School of Medicine, University of Maryland, Baltimore, Maryland.
J Trauma Acute Care Surg. 2023 May 1;94(5):718-724. doi: 10.1097/TA.0000000000003894. Epub 2023 Feb 6.
Resuscitative endovascular balloon occlusion of the aorta (REBOA) is a lifesaving therapy for hemorrhagic shock following pelvic/lower extremity injuries in military settings. However, Zone 1 aortic occlusion (AO; above the celiac artery), while providing brain/cardiac perfusion, may induce/worsen visceral ischemia and organ dysfunction. In contrast, AO Zone 3 (below the renal arteries) provides abdominal perfusion potentially minimizing ischemia/reperfusion injury. We hypothesized that, compared with AO Zone 1, AO Zone 3 provides neuro/cardioprotection while minimizing visceral ischemia and reperfusion coagulopathy after severe traumatic hemorrhage due to pelvic/lower extremity injuries.
Fifty-kilogram male Yorkshire swine underwent a blast polytrauma injury followed by a resuscitation protocol with randomization to no AO (No AO, n = 6) or AO with REBOA at Zone 1 (AO Zone 1; n = 6) or Zone 3 (AO Zone 3; n = 4). Vital signs and intracranial pressure (ICP) were monitored for 240 minutes. Citrate native and tissue plasminogen activator challenge thrombelastography, prothrombin time, creatinine, lipase, total bilirubin, troponin, and enzyme-linked immunosorbent assays protein levels were measured at set intervals.
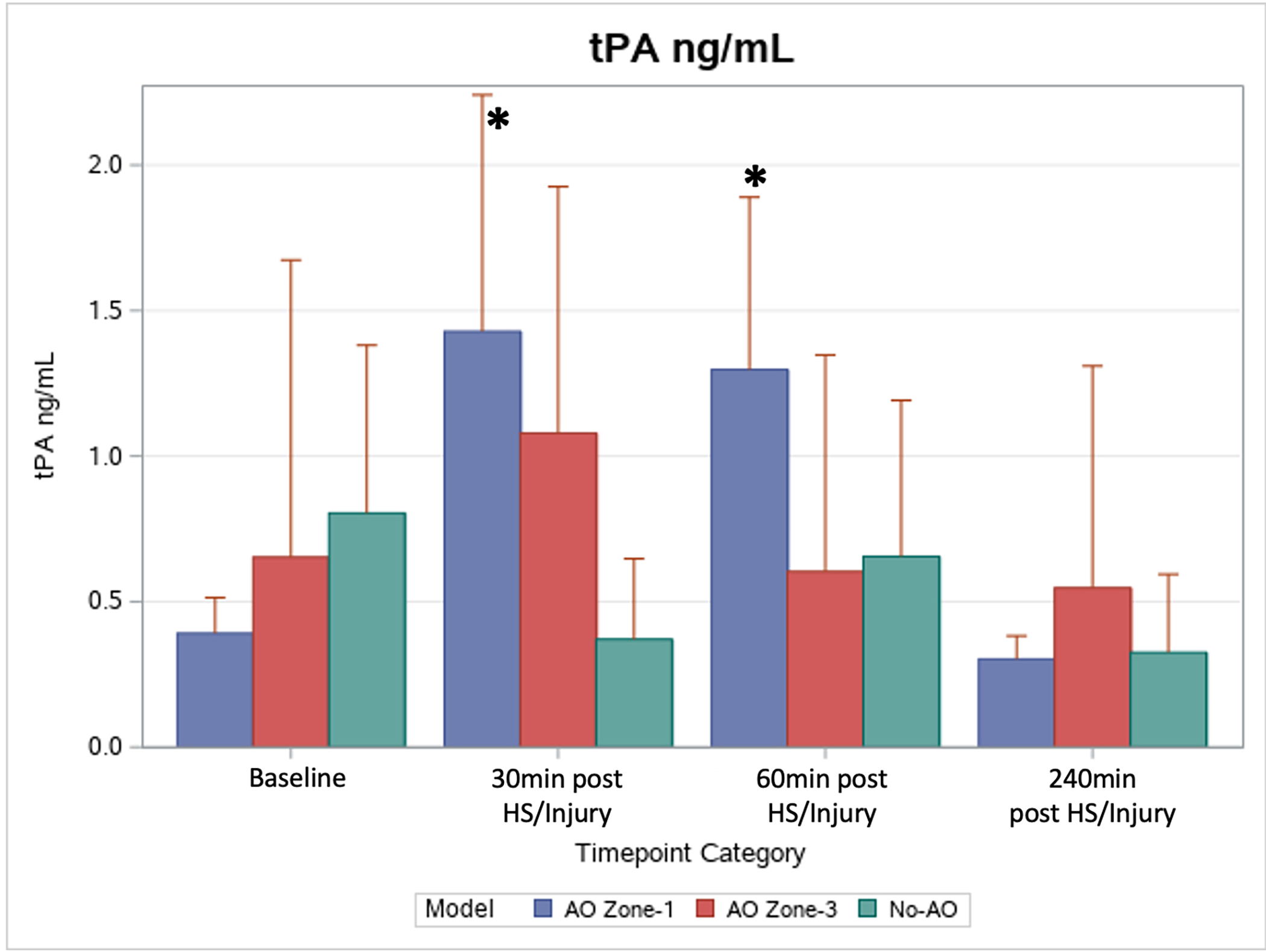
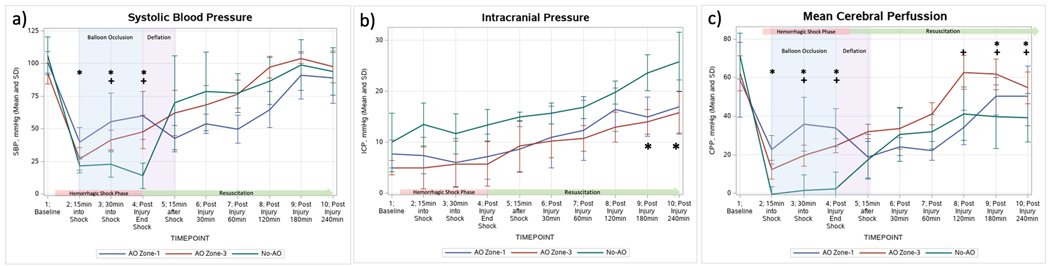
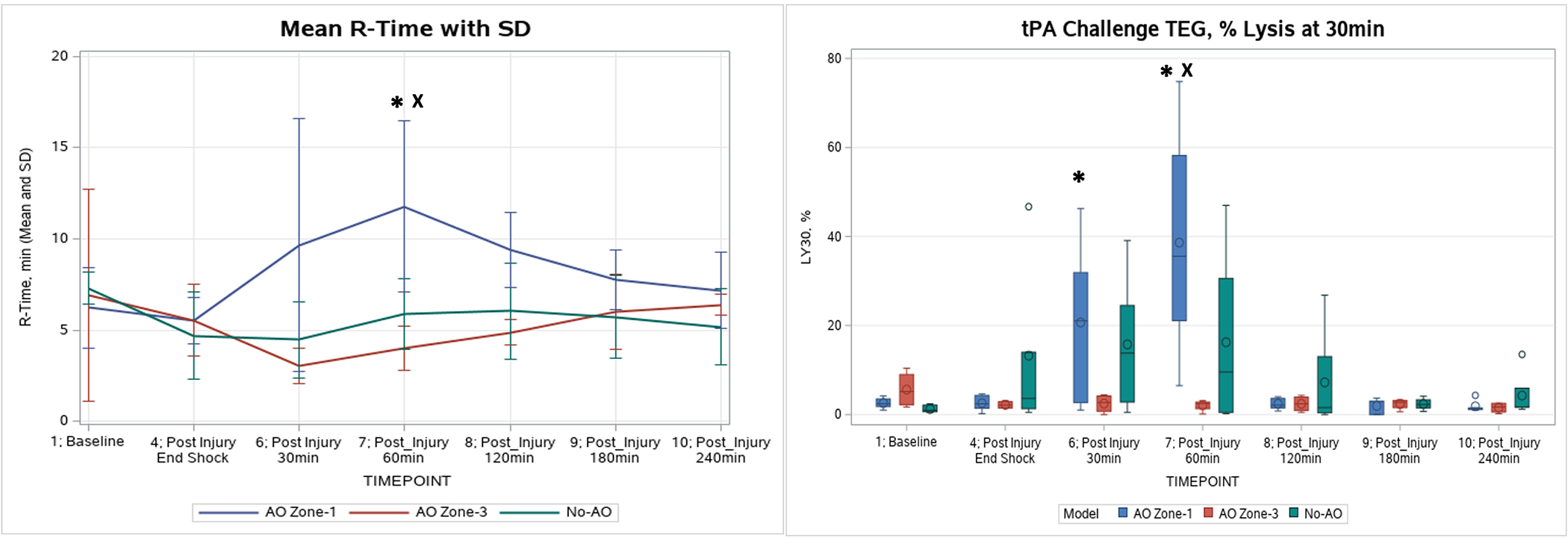
Both AO groups had significant increases in mean arterial pressure during aortic occlusion. All three groups had significant increases in ICP, but final ICP in the No AO group (26 ± 5.8 mm Hg) was significantly elevated compared with AO Zone 1 (17 ± 5.2 mm Hg) and AO Zone 3 (16 ± 4.2 mm Hg) ( p < 0.01). The final mean troponin in the No AO group (4.10 ± 5.67 ng/mL) was significantly higher than baseline (0.03 ± 0.02 ng/mL, p < 0.05), while the two AO groups had no significant changes ( p > 0.05). AO Zone 1 was the only group associated with hyperfibrinolysis ( p < 0.05) and significantly increased prothrombin time ( p < 0.05). Only AO Zone 1 group had significantly higher markers of organ damage.
Compared with AO Zone 1, AO Zone 3 provided similar neuro/cardioprotection but with less organ dysfunction and coagulopathy. This study suggests that Zone 3 REBOA may be preferable over Zone 1 for treating military relevant blast polytrauma with minimal intra-abdominal and chest trauma, but further clinical investigation is warranted.
在军事环境中,对于骨盆/下肢损伤导致的出血性休克,主动脉球囊阻断复苏术(REBOA)是一种救生治疗方法。然而,主动脉区 1 段(AO;腹腔干动脉以上)阻断虽然提供了脑/心灌注,但可能会引起/加重内脏缺血和器官功能障碍。相比之下,AO 区 3 段(肾动脉以下)阻断提供了腹部灌注,最大限度地减少了缺血/再灌注损伤。我们假设,与 AO 区 1 段相比,AO 区 3 段在骨盆/下肢损伤导致的严重创伤性出血后提供神经/心脏保护,同时最大限度地减少内脏缺血和再灌注凝血障碍。
50 公斤雄性约克郡猪经历了爆炸多发伤损伤,随后进行了复苏方案的随机分组,包括无 AO(无 AO,n=6)或 AO 区 1(AO 区 1,n=6)或 AO 区 3(AO 区 3,n=4)的 REBOA。监测 240 分钟的生命体征和颅内压(ICP)。每隔一定时间测量柠檬酸天然和组织纤溶酶原激活物挑战血栓弹性图、凝血酶原时间、肌酐、脂肪酶、总胆红素、肌钙蛋白和酶联免疫吸附试验蛋白水平。
两组 AO 患者在主动脉阻断期间的平均动脉压均显著升高。三组患者的 ICP 均显著升高,但无 AO 组的最终 ICP(26±5.8mmHg)明显高于 AO 区 1 组(17±5.2mmHg)和 AO 区 3 组(16±4.2mmHg)(p<0.01)。无 AO 组的最终平均肌钙蛋白(4.10±5.67ng/ml)明显高于基线(0.03±0.02ng/ml,p<0.05),而两组 AO 患者无明显变化(p>0.05)。只有 AO 区 1 组发生明显的纤溶亢进(p<0.05)和显著的凝血酶原时间延长(p<0.05)。只有 AO 区 1 组有明显的器官损伤标志物升高。
与 AO 区 1 相比,AO 区 3 提供了类似的神经/心脏保护,但器官功能障碍和凝血障碍较少。本研究表明,对于与军事相关的爆炸多发伤,最小化腹部和胸部创伤时,AO 区 3 段 REBOA 可能优于 AO 区 1 段,但需要进一步的临床研究。