MMWR Morb Mortal Wkly Rep. 2023 Feb 10;72(6):145-152. doi: 10.15585/mmwr.mm7206a3.
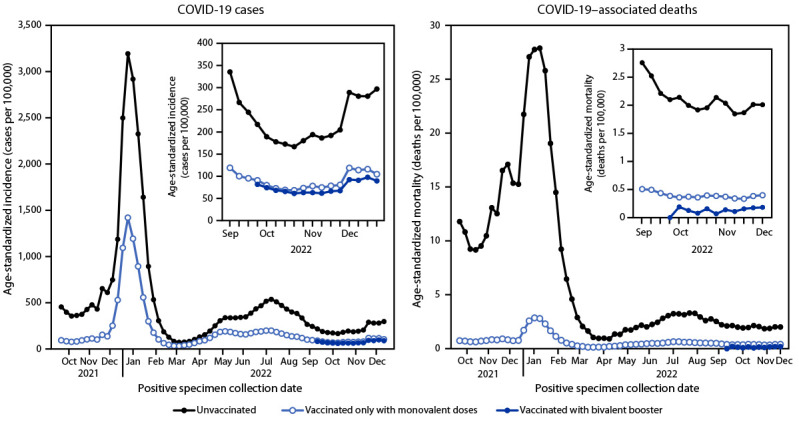
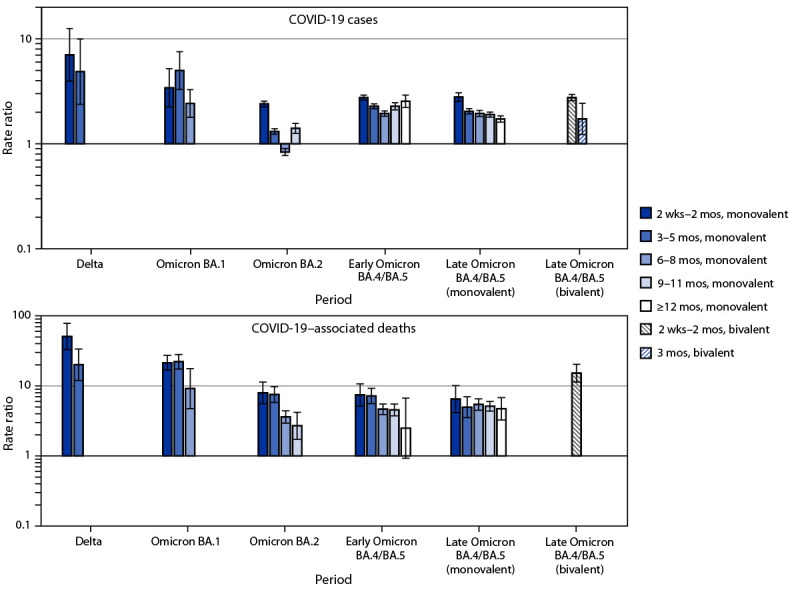
On September 1, 2022, CDC recommended an updated (bivalent) COVID-19 vaccine booster to help restore waning protection conferred by previous vaccination and broaden protection against emerging variants for persons aged ≥12 years (subsequently extended to persons aged ≥6 months).* To assess the impact of original (monovalent) COVID-19 vaccines and bivalent boosters, case and mortality rate ratios (RRs) were estimated comparing unvaccinated and vaccinated persons aged ≥12 years by overall receipt of and by time since booster vaccination (monovalent or bivalent) during Delta variant and Omicron sublineage (BA.1, BA.2, early BA.4/BA.5, and late BA.4/BA.5) predominance. During the late BA.4/BA.5 period, unvaccinated persons had higher COVID-19 mortality and infection rates than persons receiving bivalent doses (mortality RR = 14.1 and infection RR = 2.8) and to a lesser extent persons vaccinated with only monovalent doses (mortality RR = 5.4 and infection RR = 2.5). Among older adults, mortality rates among unvaccinated persons were significantly higher than among those who had received a bivalent booster (65-79 years; RR = 23.7 and ≥80 years; 10.3) or a monovalent booster (65-79 years; 8.3 and ≥80 years; 4.2). In a second analysis stratified by time since booster vaccination, there was a progressive decline from the Delta period (RR = 50.7) to the early BA.4/BA.5 period (7.4) in relative COVID-19 mortality rates among unvaccinated persons compared with persons receiving who had received a monovalent booster within 2 weeks-2 months. During the early BA.4/BA.5 period, declines in relative mortality rates were observed at 6-8 (RR = 4.6), 9-11 (4.5), and ≥12 (2.5) months after receiving a monovalent booster. In contrast, bivalent boosters received during the preceding 2 weeks-2 months improved protection against death (RR = 15.2) during the late BA.4/BA.5 period. In both analyses, when compared with unvaccinated persons, persons who had received bivalent boosters were provided additional protection against death over monovalent doses or monovalent boosters. Restored protection was highest in older adults. All persons should stay up to date with COVID-19 vaccination, including receipt of a bivalent booster by eligible persons, to reduce the risk for severe COVID-19.
2022 年 9 月 1 日,CDC 建议更新(二价)COVID-19 疫苗加强针,以帮助恢复先前接种疫苗带来的保护力减弱,并扩大对新兴变异株的保护,适用人群为年龄≥12 岁的人群(随后扩大至年龄≥6 个月的人群)。*为评估原始(单价)COVID-19 疫苗和二价加强针的效果,通过比较 Delta 变异株和 Omicron 亚谱系(BA.1、BA.2、早期 BA.4/BA.5 和晚期 BA.4/BA.5)流行期间,比较≥12 岁人群中未接种疫苗者和接种疫苗者中,整体接种疫苗者和接种加强针(单价或二价)后时间的病例和死亡率比值(RR),来评估其效果。在晚期 BA.4/BA.5 期间,未接种疫苗者的 COVID-19 死亡率和感染率高于接种二价疫苗者(死亡率 RR=14.1,感染率 RR=2.8),略低于仅接种单价疫苗者(死亡率 RR=5.4,感染率 RR=2.5)。在老年人中,未接种疫苗者的死亡率明显高于接种二价加强针者(65-79 岁;RR=23.7;≥80 岁;10.3)或接种单价加强针者(65-79 岁;8.3;≥80 岁;4.2)。在按加强针接种后时间分层的二次分析中,与接种单价疫苗者相比,未接种疫苗者的 COVID-19 死亡率相对比率从 Delta 期(RR=50.7)到早期 BA.4/BA.5 期(7.4)呈逐渐下降趋势。在早期 BA.4/BA.5 期间,在接种单价疫苗后 6-8(RR=4.6)、9-11(RR=4.5)和≥12(RR=2.5)个月时,观察到相对死亡率下降。相比之下,在过去 2 周-2 个月内接种二价加强针可提高对死亡的保护(RR=15.2)。在这两种分析中,与未接种疫苗者相比,接种二价加强针者的死亡保护效果优于单价疫苗或单价加强针。在老年人中,恢复的保护作用最强。所有人都应及时接种 COVID-19 疫苗,包括符合条件者接种二价加强针,以降低患严重 COVID-19 的风险。