Department of Medical Science, Uppsala University, Uppsala, 751 85, Sweden.
Department of Cardiology, School of Medical Sciences, Faculty of Medicine and Health, Örebro University, Örebro, SE-701 82, Sweden.
Europace. 2023 Mar 30;25(3):845-854. doi: 10.1093/europace/euad023.
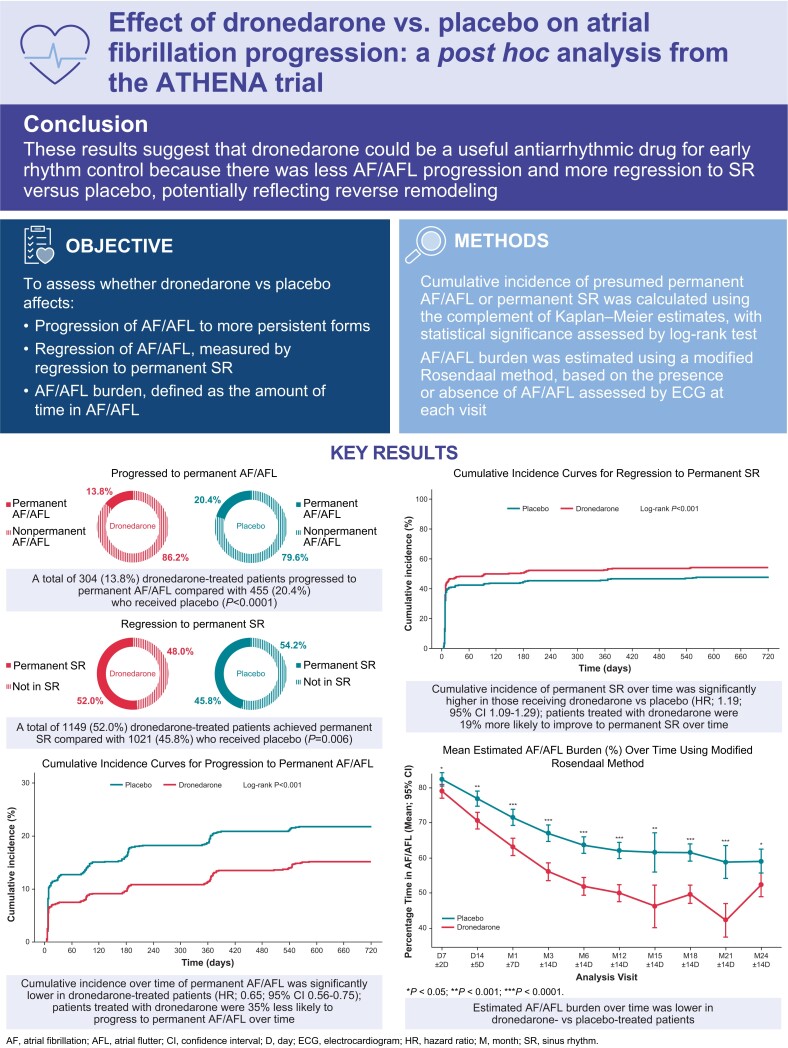
This post hoc analysis of the ATHENA trial (NCT00174785) assessed the effect of dronedarone on the estimated burden of atrial fibrillation (AF)/atrial flutter (AFL) progression to presumed permanent AF/AFL, and regression to sinus rhythm (SR), compared with placebo.
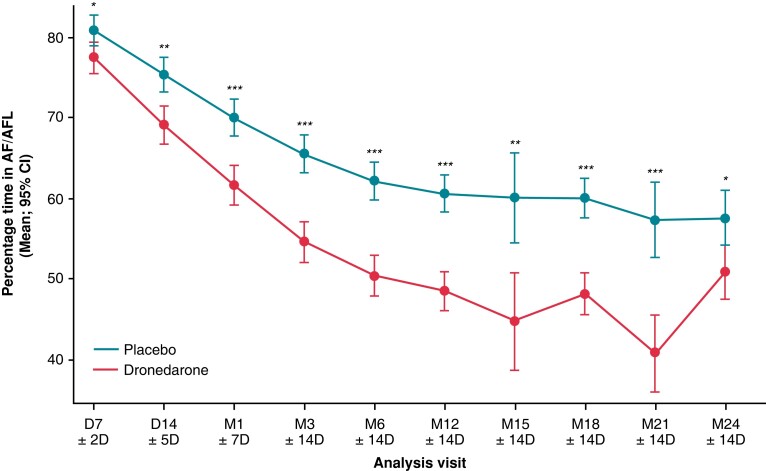
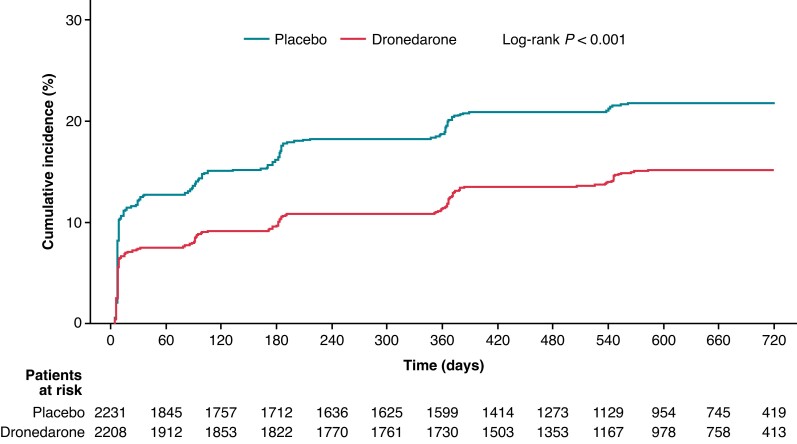
The burden of AF/AFL was estimated by a modified Rosendaal method using available electrocardiograms (ECG). Cumulative incidence of permanent AF/AFL (defined as ≥6 months of AF/AFL until end of study) or permanent SR (defined as ≥6 months of SR until end of study) were calculated using Kaplan-Meier estimates. A log-rank test was used to assess statistical significance. Hazard ratios (HRs) with corresponding 95% confidence intervals (CIs) were estimated using a Cox model, adjusted for treatment group. Of the 4439 patients included in this analysis, 2208 received dronedarone, and 2231 placebo. Baseline and clinical characteristics were well balanced between groups. Overall, 304 (13.8%) dronedarone-treated patients progressed to permanent AF/AFL compared with 455 (20.4%) treated with placebo (P < 0.0001). Compared with those receiving placebo, patients receiving dronedarone had a lower cumulative incidence of permanent AF/AFL (log-rank P < 0.001; HR: 0.65; 95% CI: 0.56-0.75), a higher cumulative incidence of permanent SR (log-rank P < 0.001; HR: 1.19; 95% CI: 1.09-1.29), and a lower estimated AF/AFL burden over time (P < 0.01 from Day 14 to Month 21).
These results suggest that dronedarone could be a useful antiarrhythmic drug for early rhythm control due to less AF/AFL progression and more regression to SR vs. placebo, potentially reflecting reverse remodeling.
NCT00174785.
本 ATHENA 试验(NCT00174785)事后分析评估了多非利特相对于安慰剂在估计的心房颤动(AF)/心房扑动(AFL)进展为假定永久性 AF/AFL 以及向窦性节律(SR)的回归方面的负担。
通过使用现有心电图(ECG)的改良 Rosendaal 方法来评估 AF/AFL 的负担。使用 Kaplan-Meier 估计值计算永久性 AF/AFL(定义为 AF/AFL ≥6 个月直至研究结束)或永久性 SR(定义为 SR ≥6 个月直至研究结束)的累积发生率。对数秩检验用于评估统计学意义。使用 Cox 模型估计风险比(HR)及其相应的 95%置信区间(CI),并根据治疗组进行调整。在这项分析中,共纳入 4439 例患者,其中 2208 例接受多非利特治疗,2231 例接受安慰剂治疗。两组患者的基线和临床特征均衡。总体而言,与接受安慰剂治疗的患者相比,304 例(13.8%)接受多非利特治疗的患者进展为永久性 AF/AFL(P<0.0001)。与接受安慰剂治疗的患者相比,接受多非利特治疗的患者永久性 AF/AFL 的累积发生率较低(对数秩 P<0.001;HR:0.65;95%CI:0.56-0.75),永久性 SR 的累积发生率较高(对数秩 P<0.001;HR:1.19;95%CI:1.09-1.29),并且随着时间的推移,AF/AFL 负担的估计值较低(从第 14 天到第 21 天,P<0.01)。
这些结果表明,多非利特可能是一种有用的抗心律失常药物,用于早期节律控制,因为与安慰剂相比,AF/AFL 进展较少,向 SR 的回归更多,这可能反映了逆重构。
NCT00174785。