Sachsska Children and Youth Hospital, Stockholm, Sweden.
Department of Anesthesia and Intensive Care, Södersjukhuset, Stockholm, Sweden.
Pediatr Res. 2023 Oct;94(4):1373-1379. doi: 10.1038/s41390-023-02509-1. Epub 2023 Feb 9.
Hospital-acquired hyponatremia remains a feared event in patients receiving hypotonic fluid therapy. Our objectives were to assess post-operative plasma-sodium concentration and to provide a physiological explanation for plasma-sodium levels over time in children with acute appendicitis.
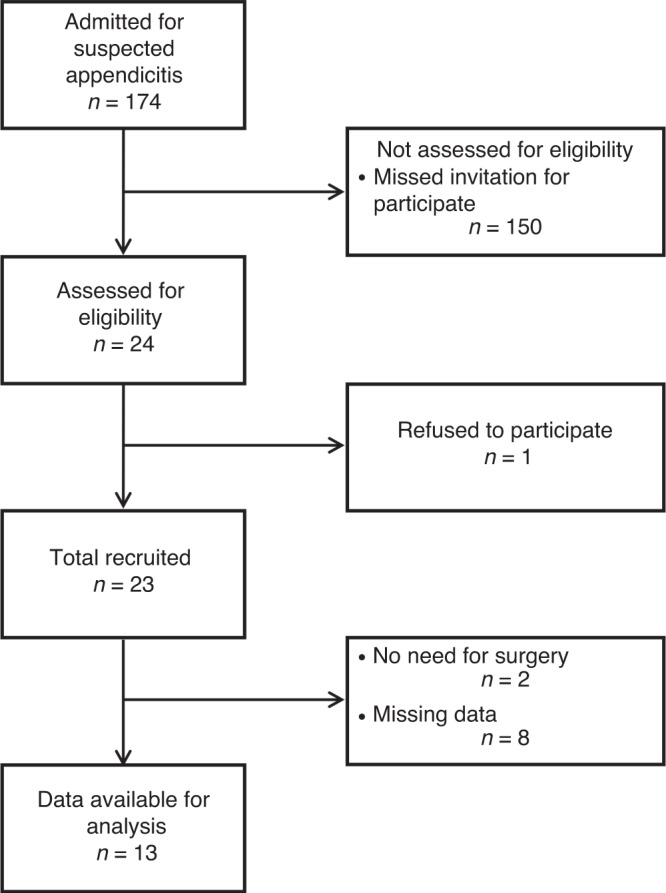
Thirteen normonatremic (plasma-sodium ≥135 mmol/L) children (8 males), median age 12.3 (IQR 11.5-13.5) years participated in this prospective observational study (ACTRN12621000587808). Urine was collected and analyzed. Blood tests, including renin, aldosterone, arginine-vasopressin, and circulating nitric oxide substrates were determined on admission, at induction of anesthesia, and at the end of surgery.
On admission, participants were assumed to be mildly dehydrated and were prescribed 50 mL/kg of Ringer's acetate intravenously followed by half-isotonic saline as maintenance fluid therapy. Blood tests, urinary indices, plasma levels of aldosterone, arginine-vasopressin, and net water-electrolyte balance indicated that participants were dehydrated on admission. Although nearly 50% of participants still had arginine-vasopressin levels that would have been expected to produce maximum antidiuresis at the end of surgery, electrolyte-free water clearance indicated that almost all participants were able to excrete net free water. No participant became hyponatremic.
The use of moderately hypotonic fluid therapy after correction of extracellular fluid deficit is not necessarily associated with post-operative hyponatremia.
Our observations show that in acutely ill normonatremic children not only the composition but also the amount of volume infused influence on the risk of hyponatremia. Our observations also suggest that perioperative administration of hypotonic fluid therapy is followed by a tendency towards hyponatremia if extracellular fluid depletion is left untreated. After correcting extracellular deficit almost all patients were able to excrete net free water. This occurred despite nearly 50% of the cohort having high circulating plasma levels of arginine-vasopressin at the end of surgery, suggesting a phenomenon of renal escape from arginine-vasopressin-induced antidiuresis.
在接受低渗液治疗的患者中,医院获得性低钠血症仍然是一种可怕的事件。我们的目的是评估术后血浆钠浓度,并为患有急性阑尾炎的儿童随时间推移的血浆钠水平提供生理学解释。
13 名血钠正常(血浆钠≥135mmol/L)的儿童(8 名男性),中位年龄 12.3(IQR 11.5-13.5)岁,参与了这项前瞻性观察研究(ACTRN12621000587808)。收集并分析尿液。入院时、麻醉诱导时和手术结束时测定血检,包括肾素、醛固酮、精氨酸加压素和循环一氧化氮底物。
入院时,参与者被认为轻度脱水,并给予 50ml/kg 的醋酸林格氏液静脉内补液,然后给予半等渗盐水作为维持液治疗。血检、尿指数、血浆醛固酮、精氨酸加压素和净水电解质平衡水平表明,参与者入院时脱水。尽管手术结束时近 50%的参与者仍有精氨酸加压素水平,预计会产生最大的抗利尿作用,但无电解质自由水清除表明,几乎所有参与者都能够排出净自由水。没有参与者出现低钠血症。
在纠正细胞外液不足后使用中度低渗液治疗不一定与术后低钠血症有关。
我们的观察表明,在急性病正常血钠的儿童中,不仅输液的组成,而且输液的量都会影响低钠血症的风险。我们的观察还表明,如果不治疗细胞外液耗竭,围手术期给予低渗液治疗后会出现低钠血症的趋势。纠正细胞外液不足后,几乎所有患者都能够排出净自由水。尽管近 50%的队列在手术结束时循环血浆精氨酸加压素水平较高,但仍出现这种情况,这表明存在一种从精氨酸加压素诱导的抗利尿作用中肾逃逸的现象。