Division of Cardiothoracic Surgery, Department of Surgery, Washington University School of Medicine, St. Louis, Missouri, USA; Division of Public Health Sciences, Department of Surgery, Washington University School of Medicine, St. Louis, Missouri, USA.
Division of Cardiothoracic Surgery, Department of Surgery, Washington University School of Medicine, St. Louis, Missouri, USA.
Am J Transplant. 2023 Apr;23(4):540-548. doi: 10.1016/j.ajt.2022.12.014. Epub 2023 Jan 3.
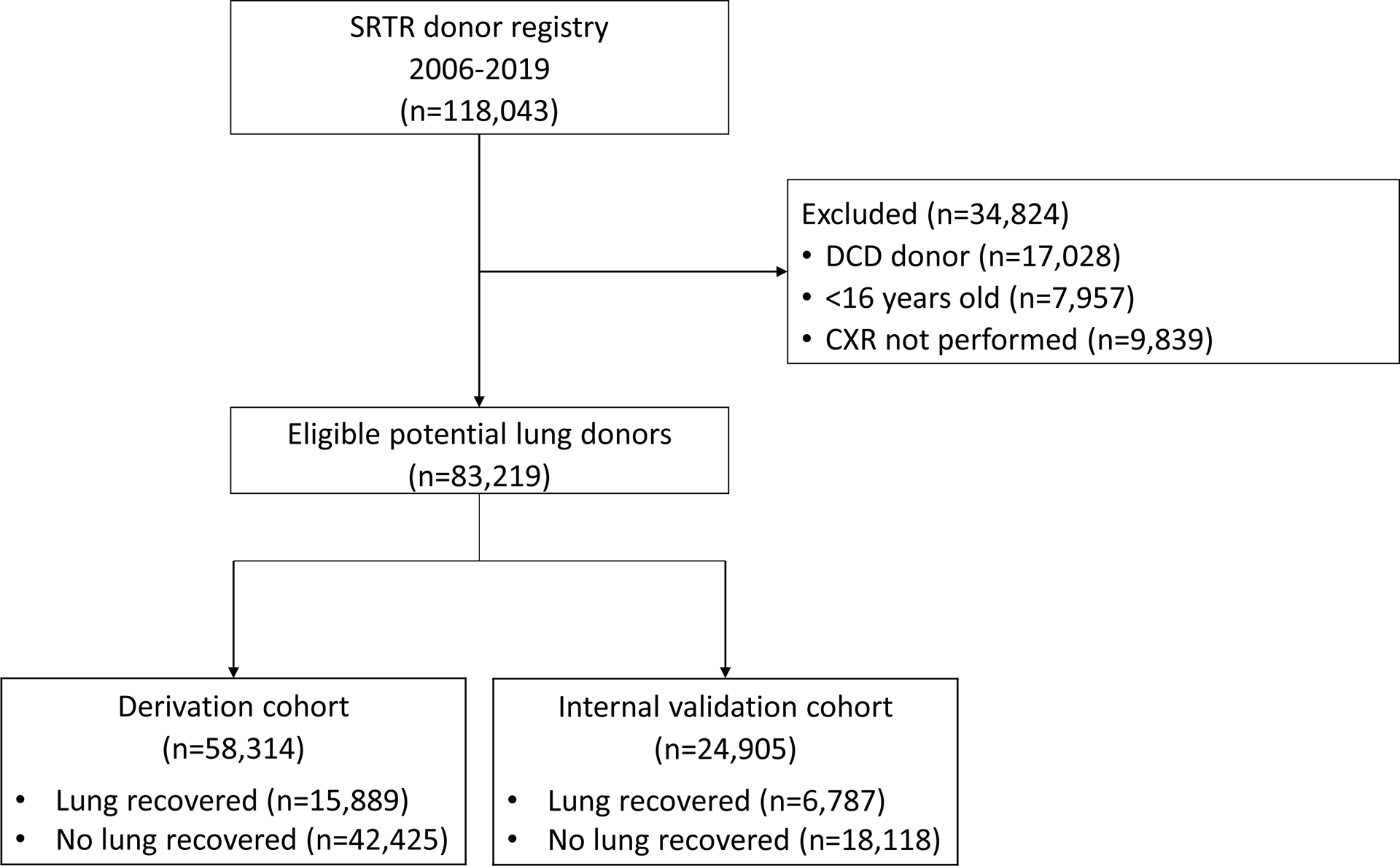
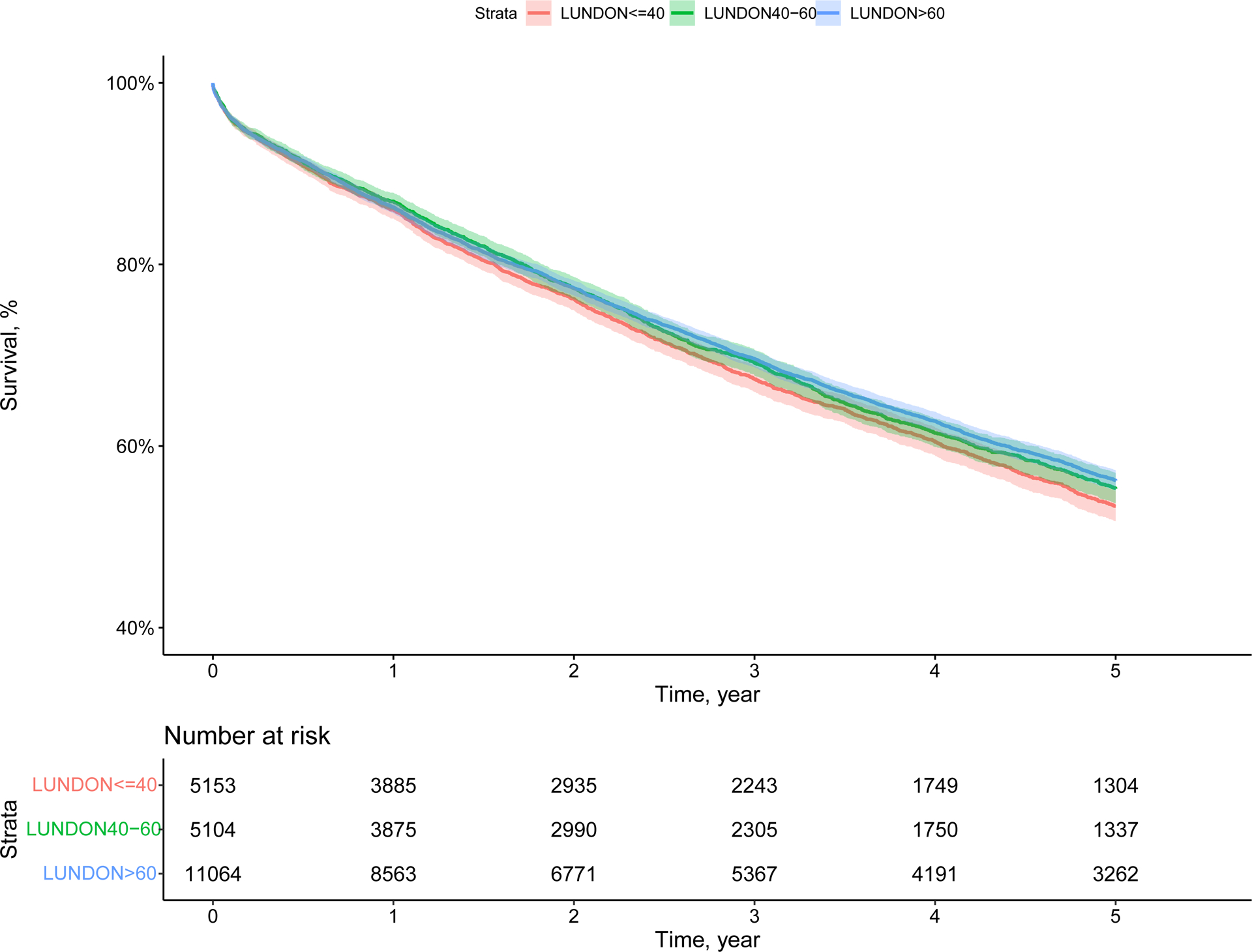
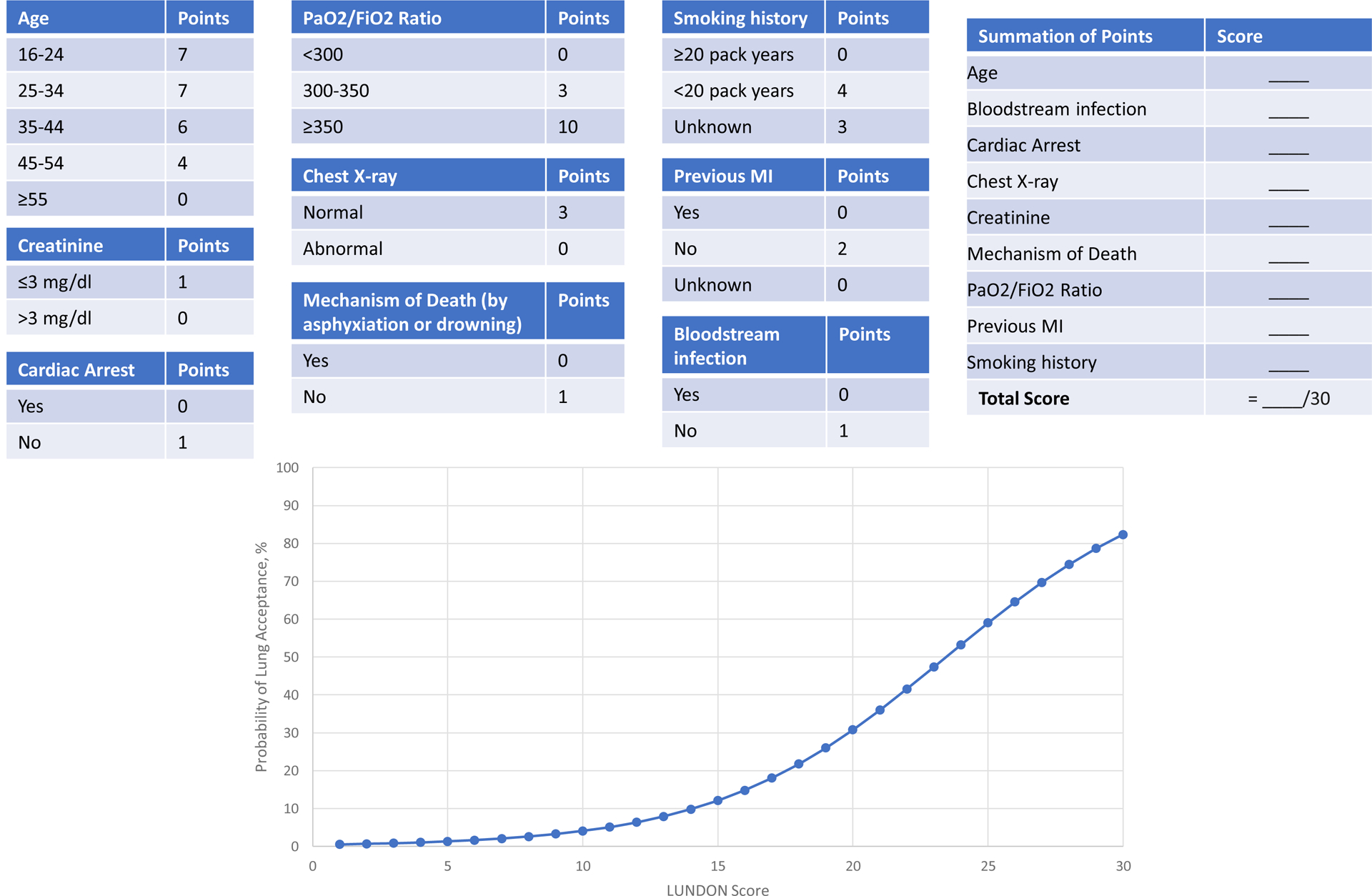
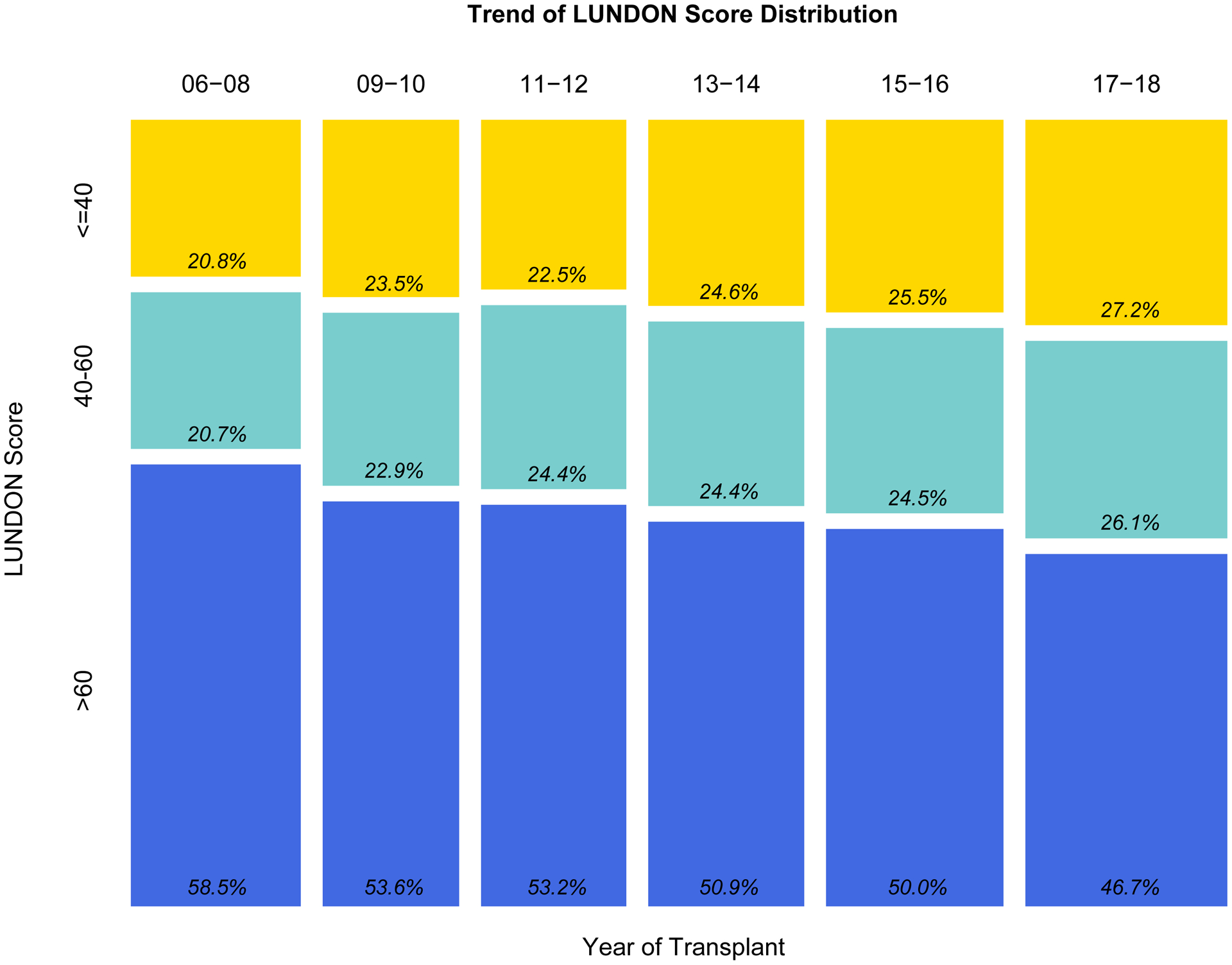
There is a chronic shortage of donor lungs for pulmonary transplantation due, in part, to low lung utilization rates in the United States. We performed a retrospective cohort study using data from the Scientific Registry of Transplant Recipients database (2006-2019) and developed the lung donor (LUNDON) acceptability score. A total of 83 219 brain-dead donors were included and were randomly divided into derivation (n = 58 314, 70%) and validation (n = 24 905, 30%) cohorts. The overall lung acceptance was 27.3% (n = 22 767). Donor factors associated with the lung acceptance were age, maximum creatinine, ratio of arterial partial pressure of oxygen to fraction of inspired oxygen, mechanism of death by asphyxiation or drowning, history of cigarette use (≥20 pack-years), history of myocardial infarction, chest x-ray appearance, bloodstream infection, and the occurrence of cardiac arrest after brain death. The prediction model had high discriminatory power (C statistic, 0.891; 95% confidence interval, 0.886-0.895) in the validation cohort. We developed a web-based, user-friendly tool (available at https://sites.wustl.edu/lundon) that provides the predicted probability of donor lung acceptance. LUNDON score was also associated with recipient survival in patients with high lung allocation scores. In conclusion, the multivariable LUNDON score uses readily available donor characteristics to reliably predict lung acceptability. Widespread adoption of this model may standardize lung donor evaluation and improve lung utilization rates.
由于美国肺部利用率低,导致用于肺移植的捐献者肺部器官长期短缺。我们使用来自移植受者科学登记处数据库的数据(2006-2019 年)进行了一项回顾性队列研究,并开发了肺供体(LUNDON)可接受性评分。共纳入 83219 例脑死亡供者,随机分为推导队列(n = 58314,70%)和验证队列(n = 24905,30%)。总体肺接受率为 27.3%(n = 22767)。与肺接受相关的供者因素包括年龄、最大肌酐、动脉部分压力与吸入氧分数的比值、窒息或溺水导致的死亡机制、吸烟史(≥20 包年)、心肌梗死史、胸部 X 线表现、血流感染和脑死亡后发生心脏骤停。该预测模型在验证队列中具有较高的区分能力(C 统计值,0.891;95%置信区间,0.886-0.895)。我们开发了一个基于网络的、用户友好的工具(可在 https://sites.wustl.edu/lundon 获得),该工具提供供者肺部接受预测概率。在高肺分配评分的患者中,LUNDON 评分也与受体生存率相关。总之,多变量 LUNDON 评分使用现成的供者特征来可靠地预测肺可接受性。该模型的广泛应用可能会使肺供者评估标准化,并提高肺部利用率。