Department of Anesthesiology, The Third People's Hospital of Chengdu, Chengdu City, China.
Medicine (Baltimore). 2023 Feb 17;102(7):e32981. doi: 10.1097/MD.0000000000032981.
Patients undergoing lumbar spine surgery usually suffer from moderate to severe acute pain. Erector spinae plane block (ESPB) has been applied to relieve acute pain in various surgeries and improve postoperative outcomes. This study aimed to further identify the efficacy and safety of erector spinae plane block in patients undergoing lumbar spine surgery. This study also evaluates the outcomes of the erector spinae plane block compared with other regional blocks.
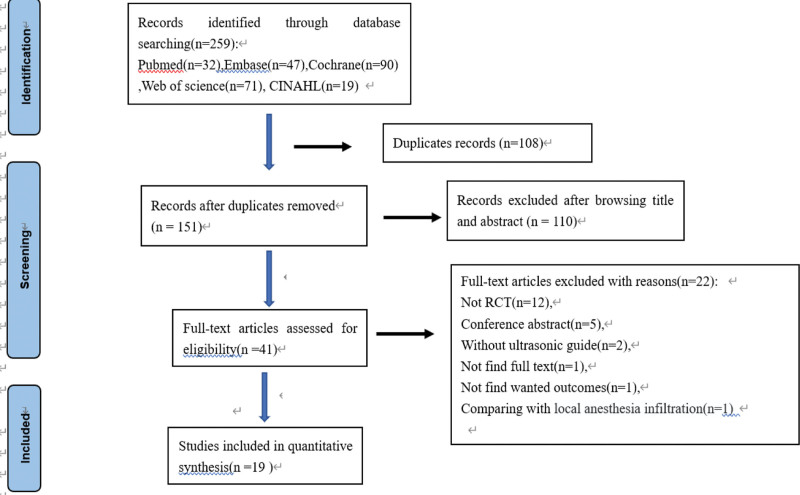
We searched PubMed, Web of Science, Cochrane library, Embase, and CINAHL databases to identify all randomized controlled trials evaluating the effects of ESPB on postoperative pain after lumbar spine surgery. The primary outcome is postoperative total opioid consumption in 24 hours. The secondary outcomes are postoperative pain scores, intraoperative opioid consumption, time to first rescue analgesia, number of patients requiring rescue analgesia, first time to ambulation after surgery, length of hospital stay, patients' satisfaction score, and postoperative side effects such as postoperative nausea and vomiting, itching.
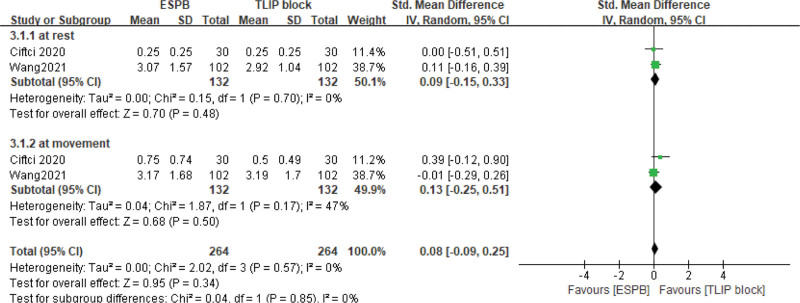
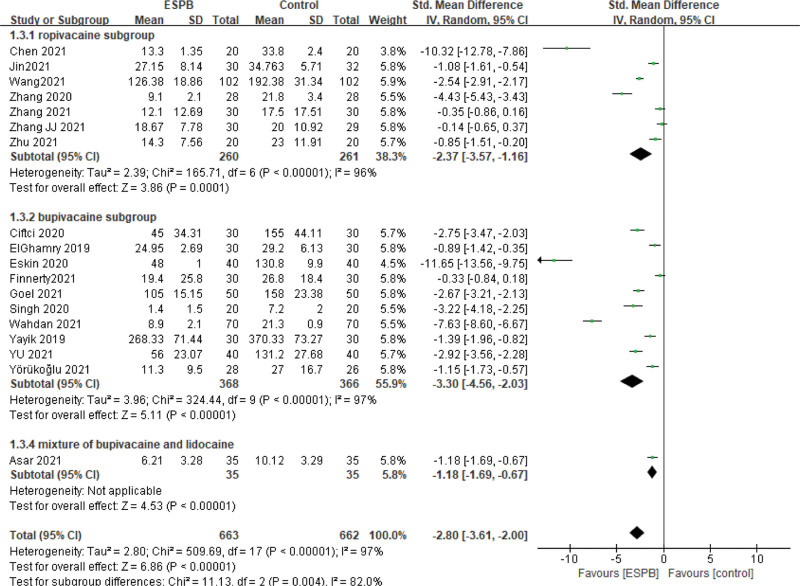
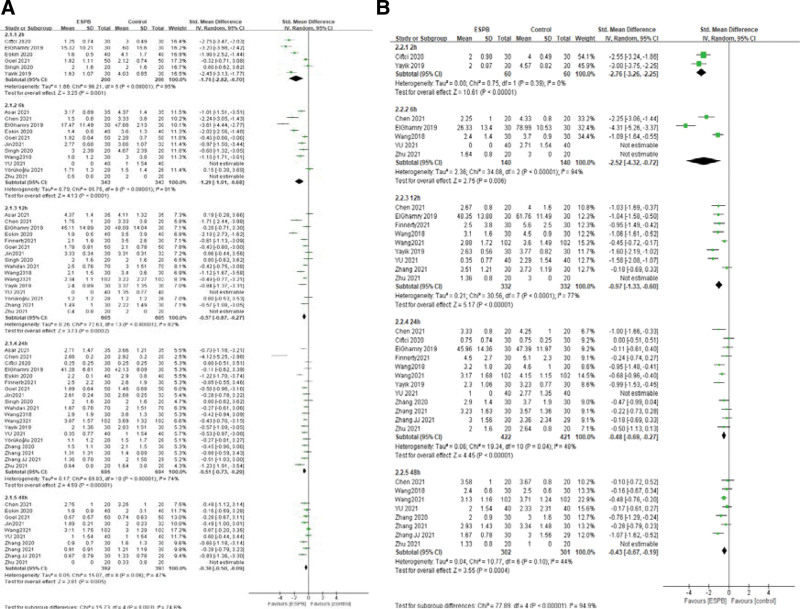
A total of 19 randomized controlled trials are included in the final analysis. Compared with no/sham block, ultrasound-guided erector spinae plane block can decrease perioperative opioid consumption including intraoperative opioid consumption: standardized mean difference (SMD) = -3.04, 95% confidence interval (CI) (-3.99, -2.09), P < .01, and opioid consumption postoperatively: (SMD = -2.80, 95% CI [-3.61, -2.00], P < .01); reduce postoperative pain at 2, 6, 12, 24, and 48 hours both at rest and movement; meanwhile shorten time to hospital length of stay: (SMD = -1.01, 95% CI [-1.72, 0.30], P = .006), decrease postoperative nausea and vomiting (RR = 0.35, 95% CI [0.27, 0.46], P < .00001), and improve patient satisfaction (SMD = -2.03, 95% CI [-0.96, 3.11], P = .0002). But ultrasound-guided ESPB doesn't shorten the time to ambulation after surgery (SMD = -0.56, 95% CI [-1.21, 0.08], P = .09). Additionally, ESPB is not superior to other regional blocks (e.g., thoracolumbar interfascial plane/midtransverse process to pleura block).
This meta-analysis demonstrates that ultrasound-guided ESPB can provide effective postoperative analgesia in patients undergoing lumbar spine surgery and improve postoperative outcomes, and it deserves to be recommended as an analgesic adjunct in patients undergoing lumbar spine surgeries.
接受腰椎手术的患者通常会遭受中度至重度急性疼痛。竖脊肌平面阻滞(ESPB)已应用于缓解各种手术中的急性疼痛,并改善术后结果。本研究旨在进一步确定 ESPB 对腰椎手术患者的疗效和安全性。本研究还评估了 ESPB 与其他区域阻滞的结果。
我们检索了 PubMed、Web of Science、Cochrane 图书馆、Embase 和 CINAHL 数据库,以确定所有评估 ESPB 对腰椎手术后术后疼痛影响的随机对照试验。主要结果是术后 24 小时内的总阿片类药物消耗量。次要结果是术后疼痛评分、术中阿片类药物消耗量、首次解救镇痛时间、需要解救镇痛的患者人数、术后首次下床时间、住院时间、患者满意度评分以及术后恶心和呕吐、瘙痒等副作用。
共有 19 项随机对照试验纳入最终分析。与无/假阻滞相比,超声引导的竖脊肌平面阻滞可以减少围手术期阿片类药物的消耗,包括术中阿片类药物的消耗:标准化均数差(SMD)=-3.04,95%置信区间(CI)(-3.99,-2.09),P<.01,和术后阿片类药物的消耗:(SMD=-2.80,95%CI[-3.61,-2.00],P<.01);降低术后 2、6、12、24 和 48 小时的静息和运动时的疼痛;同时缩短住院时间:(SMD=-1.01,95%CI[-1.72,0.30],P=0.006),减少术后恶心和呕吐(RR=0.35,95%CI[0.27,0.46],P<.00001),并提高患者满意度(SMD=-2.03,95%CI[-0.96,3.11],P=0.0002)。但是,超声引导的 ESPB 并不能缩短术后下床活动的时间(SMD=-0.56,95%CI[-1.21,0.08],P=0.09)。此外,ESPB 并不优于其他区域阻滞(例如,胸腰椎筋膜/中横突至胸膜阻滞)。
本荟萃分析表明,超声引导的 ESPB 可在腰椎手术患者中提供有效的术后镇痛,并改善术后结果,值得作为腰椎手术患者的镇痛辅助手段。