Nwana Nwabunie, Taha Mohamad B, Javed Zulqarnain, Gullapelli Rakesh, Nicolas Juan C, Jones Stephen L, Acquah Isaac, Khan Safi, Satish Priyanka, Mahajan Shivani, Cainzos-Achirica Miguel, Nasir Khurram
Center for Outcomes Research, Houston Methodist Hospital, Houston, TX, USA.
Division of Cardiovascular Prevention and Wellness, Houston Methodist DeBakey Heart and Vascular Center, Houston, TX, USA.
Prev Med Rep. 2022 Dec 24;31:102100. doi: 10.1016/j.pmedr.2022.102100. eCollection 2023 Feb.
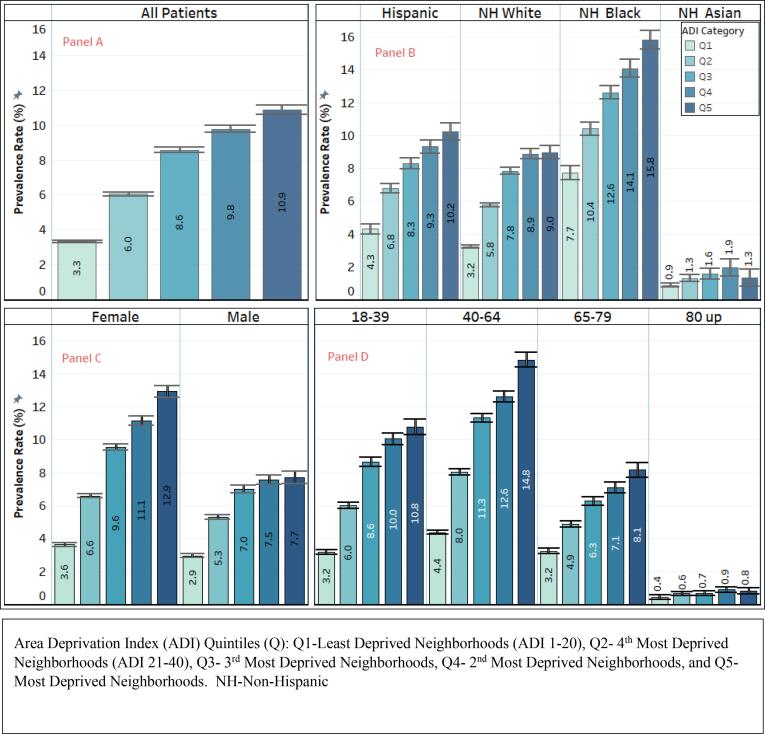
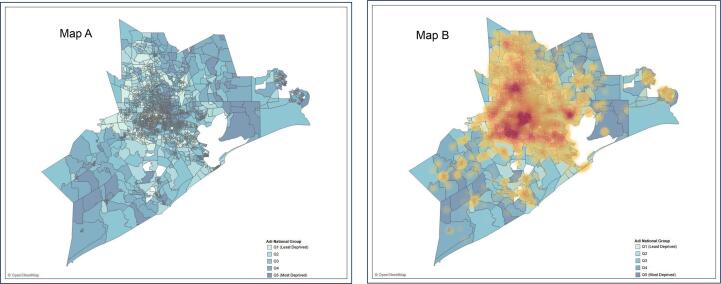
This study examined the relationship between a validated measure of socioeconomic deprivation, such as the Area Deprivation Index (ADI), and morbid obesity. We used cross-sectional data on adult patients (≥18 years) in the Houston Methodist Cardiovascular Disease Health System Learning Registry (located in Houston, Texas, USA) between June 2016 and July 2021. Each patient was grouped by quintiles of ADI, with higher quintiles signaling greater deprivation. BMI was calculated using measured height and weight with morbid obesity defined as ≥ 40 kg/m. Multivariable logistic regression models were used to examine the association between ADI and morbid obesity adjusting for demographic (age, sex, and race/ethnicity) factors. Out of the 751,174 adults with an ADI ranking included in the analysis, 6.9 % had morbid obesity (n = 51,609). Patients in the highest ADI quintile had a higher age-adjusted prevalence (10.9 % vs 3.3 %), and about 4-fold odds (aOR, 3.8; 95 % CI = 3.6, 3.9) of morbid obesity compared to the lowest ADI quintile. We tested for and found interaction effects between ADI and each demographic factor, with stronger ADI-morbid obesity association observed for patients that were female, Hispanic, non-Hispanic White and 40-65 years old. The highest ADI quintile also had a high prevalence (44 %) of any obesity (aOR, 2.2; 95 % CI = 2.1, 2.2). In geospatial mapping, areas with higher ADI were more likely to have higher proportion of patients with morbid obesity. Census-based measures, like the ADI, may be informative for area-level obesity reduction strategies as it can help identify neighborhoods at high odds of having patients with morbid obesity.
本研究探讨了一种经过验证的社会经济剥夺衡量指标,如地区剥夺指数(ADI)与病态肥胖之间的关系。我们使用了2016年6月至2021年7月期间美国德克萨斯州休斯顿卫理公会心血管疾病健康系统学习登记处中成年患者(≥18岁)的横断面数据。每位患者按ADI五分位数分组,五分位数越高表明剥夺程度越高。通过测量身高和体重计算体重指数(BMI),病态肥胖定义为BMI≥40kg/m²。使用多变量逻辑回归模型来检验ADI与病态肥胖之间的关联,并对人口统计学因素(年龄、性别和种族/族裔)进行调整。在纳入分析的751174名有ADI排名的成年人中,6.9%患有病态肥胖(n = 51609)。ADI最高五分位数的患者年龄调整患病率较高(10.9%对3.3%),与ADI最低五分位数相比,病态肥胖的几率约高4倍(调整后比值比,3.8;95%置信区间 = 3.6,3.9)。我们检验并发现了ADI与各人口统计学因素之间的交互作用,在女性、西班牙裔、非西班牙裔白人以及40 - 65岁的患者中观察到更强的ADI与病态肥胖的关联。ADI最高五分位数的任何肥胖患病率也很高(44%)(调整后比值比,2.2;95%置信区间 = 2.1,2.2)。在地理空间映射中,ADI较高的地区病态肥胖患者比例更有可能更高。基于人口普查的指标,如ADI,可能有助于制定地区层面的肥胖减少策略,因为它可以帮助识别病态肥胖患者几率较高的社区。