Department of Health Sciences Research, Mayo Clinic, 200 First Street SW, Rochester, MN, 55905, USA.
Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery, Mayo Clinic, 200 First Street SW, Rochester, MN, 55905, USA.
BMC Public Health. 2020 Jan 6;20(1):13. doi: 10.1186/s12889-019-8123-0.
Persons with low socioeconomic status may be disproportionately at risk for multimorbidity.
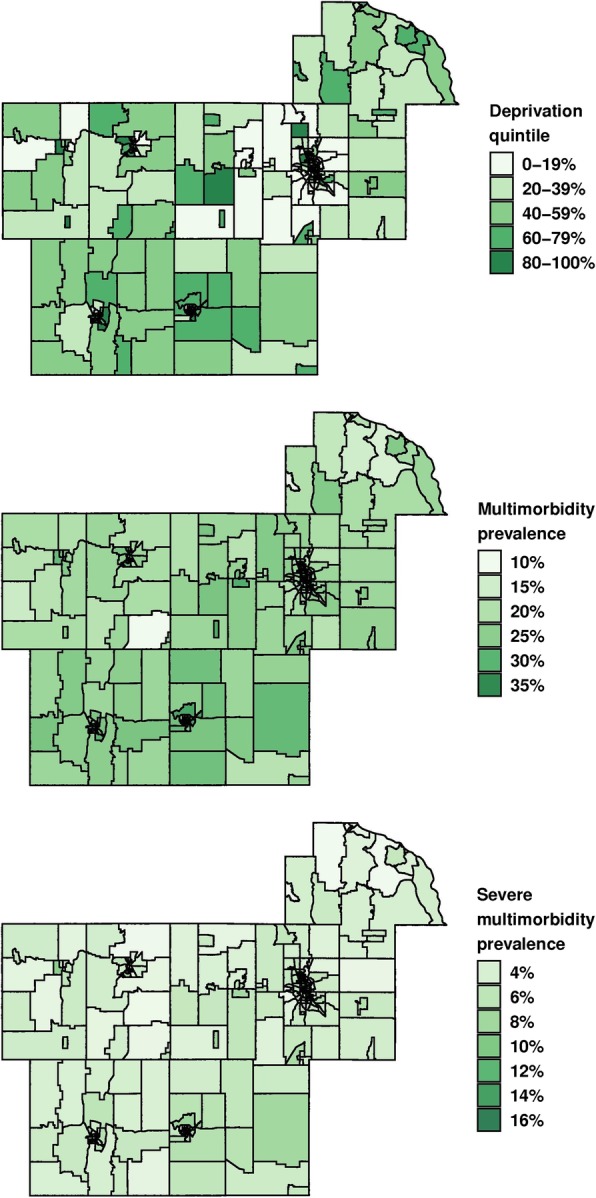
Adults aged ≥20 years on 4/1/2015 from 7 counties in Minnesota were identified using the Rochester Epidemiology Project (population-based sample). A composite measure of neighborhood socioeconomic disadvantage, the area deprivation index (ADI), was estimated at the census block group level (n = 251). The prevalence of 21 chronic conditions was obtained to calculate the proportion of persons with multimorbidity (≥2 chronic conditions) and severe multimorbidity (≥5 chronic conditions). Hierarchical logistic regression was used to estimate the association of ADI with multimorbidity and severe multimorbidity using odds ratios (OR).
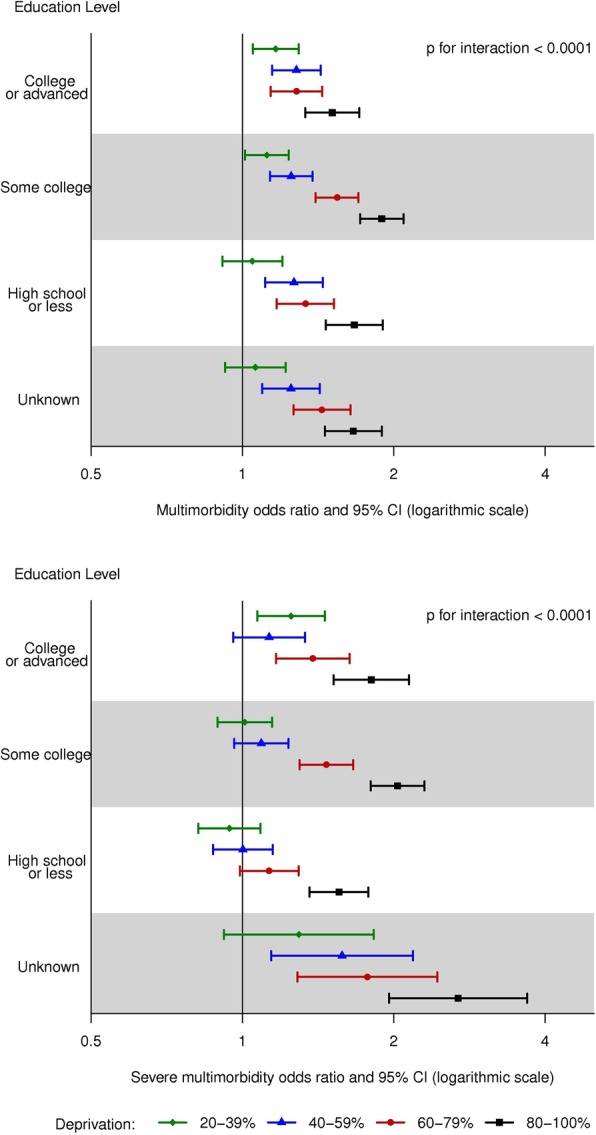
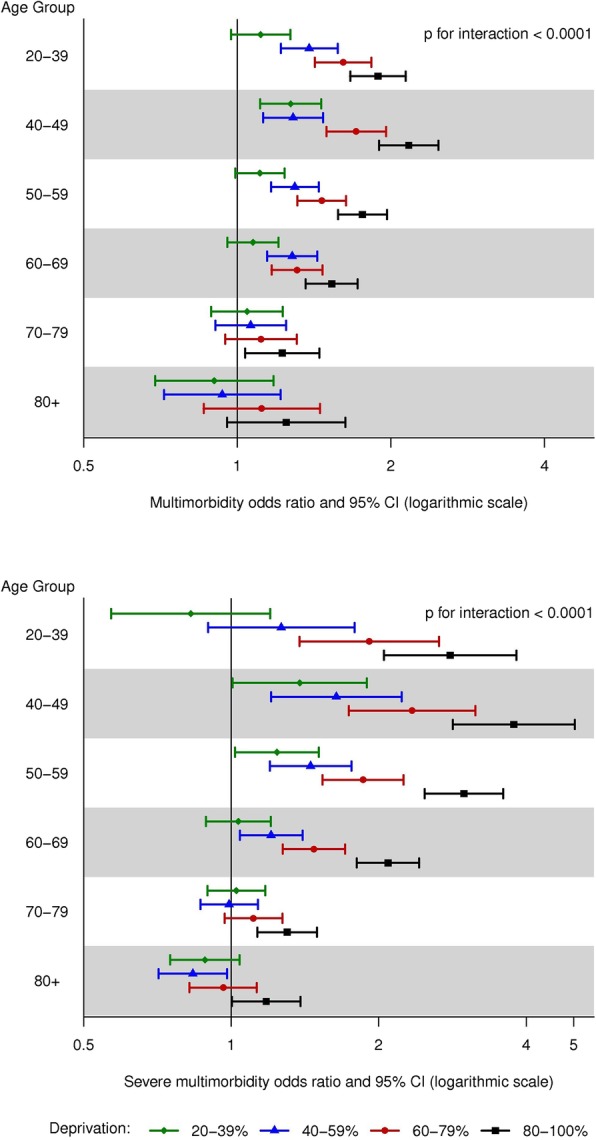
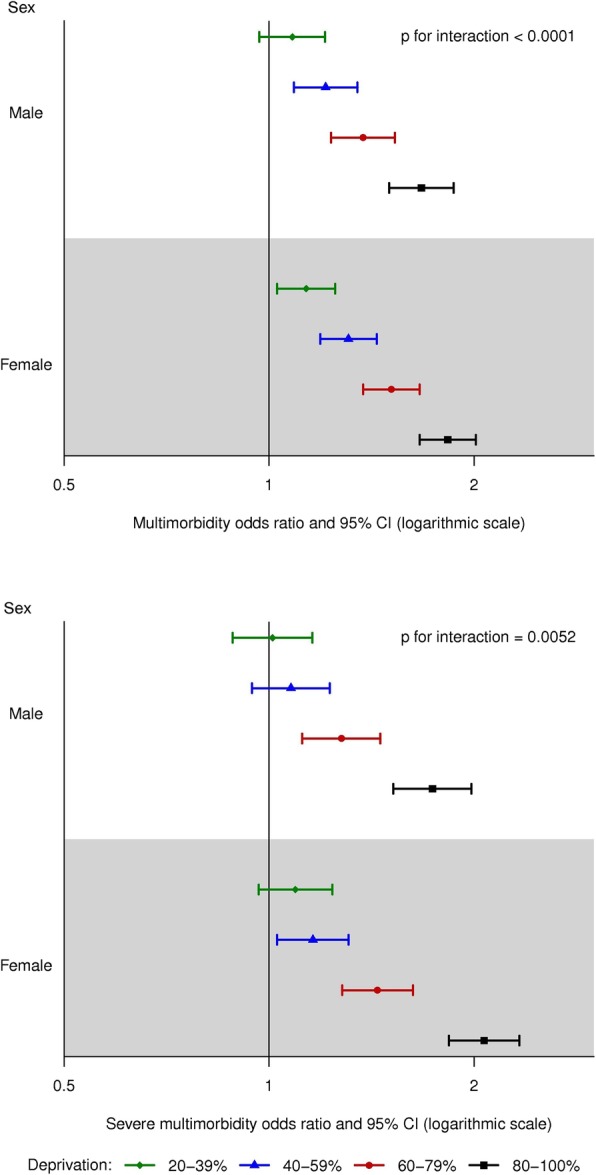
Among 198,941 persons (46.7% male, 30.6% aged ≥60 years), the age- and sex-standardized (to the United States 2010 census) median prevalence (Q1, Q3) was 23.4% (21.3%, 25.9%) for multimorbidity and 4.8% (4.0%, 5.7%) for severe multimorbidity. Compared with persons in the lowest quintile of ADI, persons in the highest quintile had a 50% increased risk of multimorbidity (OR 1.50, 95% CI 1.39-1.62) and a 67% increased risk of severe multimorbidity (OR 1.67, 95% CI 1.51-1.86) after adjusting for age, sex, race, and ethnicity. Associations were stronger after further adjustment for individual level of education; persons in the highest quintile had a 78% increased risk of multimorbidity (OR 1.78, 95% CI 1.62-1.96) and a 92% increased risk of severe multimorbidity (OR 1.92, 95% CI 1.72-2.13). There was evidence of interactions between ADI and age, between ADI and sex, and between ADI and education. After age 70 years, no difference in the risk of multimorbidity was observed across quintiles of ADI. The pattern of increasing multimorbidity with increasing ADI was more pronounced in women. Finally, there was less variability across quintiles of ADI for the most highly educated group.
Higher ADI was associated with increased risk of multimorbidity, and the associations were strengthened after adjustment for individual level of education, suggesting that neighborhood context plays a role in health above and beyond individual measures of socioeconomic status. Furthermore, associations were more pronounced in younger persons and women, highlighting the importance of interventions to prevent chronic conditions in younger women, in particular.
社会经济地位较低的人群可能面临更高的多种疾病风险。
2015 年 4 月 1 日,从明尼苏达州的 7 个县中选取了年龄≥20 岁的成年人(基于人群的样本),使用罗切斯特流行病学项目进行识别。使用社区剥夺指数(ADI)对邻里社会经济劣势进行综合评估,ADI 是在普查块组层面估计的(n=251)。为了计算多种疾病(≥2 种慢性疾病)和严重多种疾病(≥5 种慢性疾病)的患病率,获得了 21 种慢性疾病的患病率。使用优势比(OR),通过分层逻辑回归估计 ADI 与多种疾病和严重多种疾病的关联。
在 198941 名参与者中(46.7%为男性,30.6%年龄≥60 岁),年龄和性别标准化(至 2010 年美国人口普查)的中位数患病率(Q1,Q3)为 23.4%(21.3%,25.9%)为多种疾病,4.8%(4.0%,5.7%)为严重多种疾病。与 ADI 最低五分位数的参与者相比,ADI 最高五分位数的参与者的多种疾病风险增加了 50%(OR 1.50,95%CI 1.39-1.62),严重多种疾病的风险增加了 67%(OR 1.67,95%CI 1.51-1.86),在调整了年龄、性别、种族和民族之后。进一步调整个体教育水平后,关联更加强烈;ADI 最高五分位数的参与者的多种疾病风险增加了 78%(OR 1.78,95%CI 1.62-1.96),严重多种疾病的风险增加了 92%(OR 1.92,95%CI 1.72-2.13)。ADI 与年龄、ADI 与性别以及 ADI 与教育之间存在交互作用的证据。70 岁以后,ADI 五分位数之间的多种疾病风险没有差异。随着 ADI 的增加,多种疾病的风险呈上升趋势,在女性中更为明显。最后,在受教育程度最高的群体中,ADI 五分位数之间的差异较小。
较高的 ADI 与多种疾病风险增加有关,并且在调整个体教育水平后,这种关联得到了加强,这表明邻里环境在个体社会经济地位指标之外对健康也有影响。此外,在年轻人和女性中,关联更加明显,突出了针对年轻女性预防慢性疾病的干预措施的重要性。