Lombardi Conner V, Lang Jacob J, Li Meng-Hao, Siddique Abu Bakkar, Koizumi Naoru, Ekwenna Obi
Department of Urology and Transplantation, University of Toledo College of Medicine and Life Sciences, Toledo, OH 43614, USA.
Schar School of Policy and Government, George Mason University, Fairfax, VA 22030, USA.
Healthcare (Basel). 2023 Feb 18;11(4):612. doi: 10.3390/healthcare11040612.
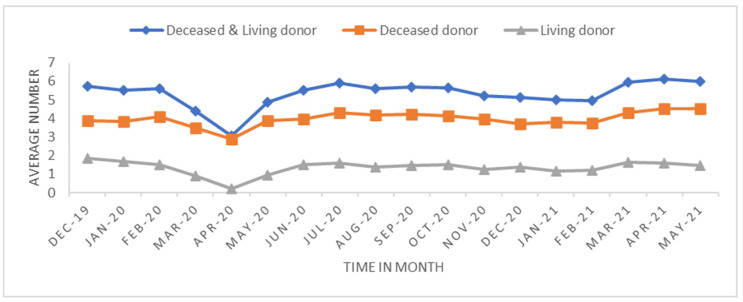
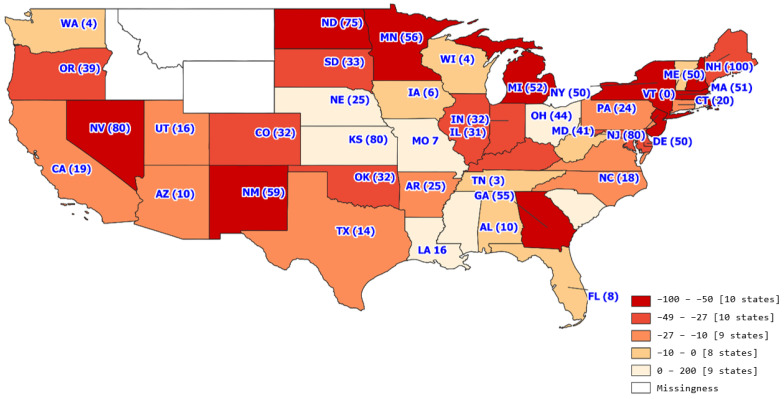
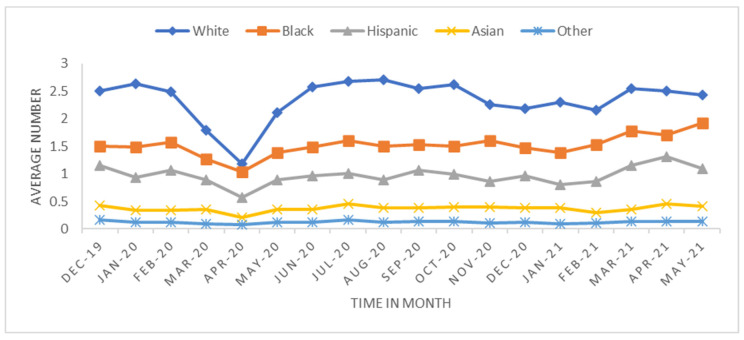
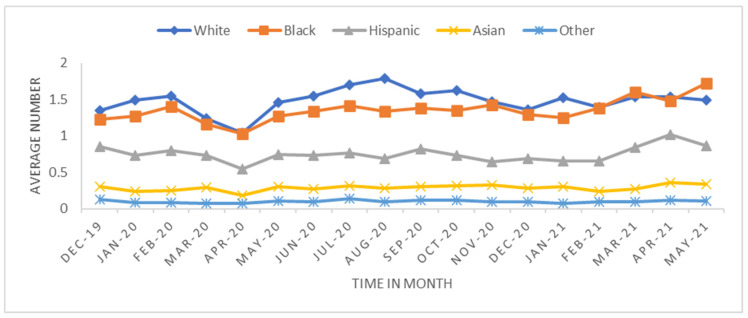
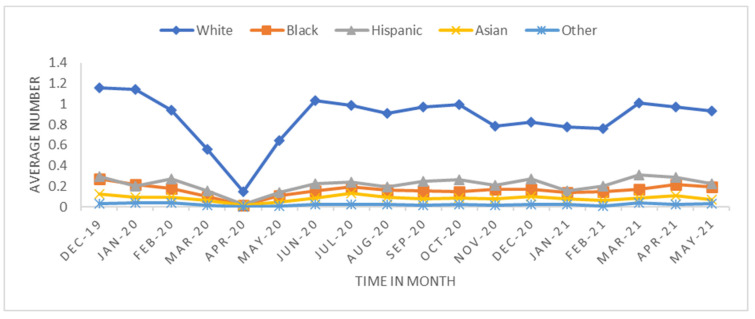
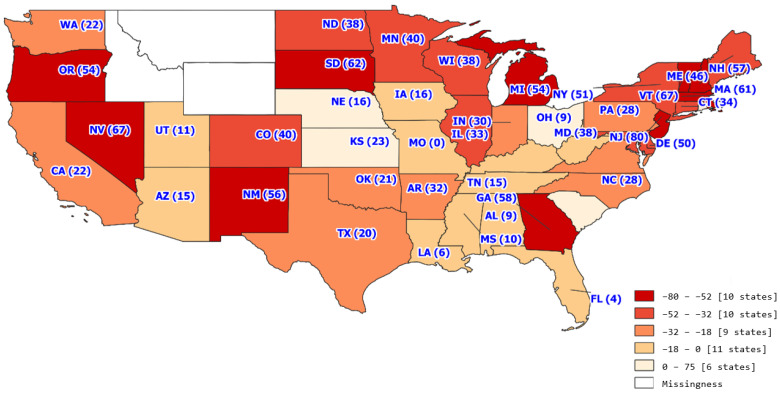
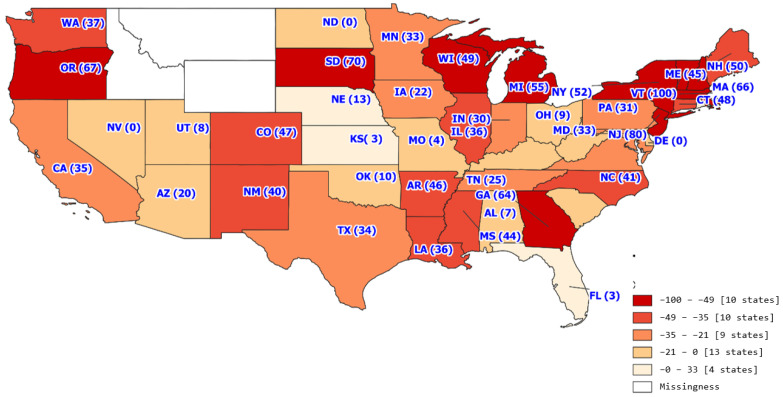
The primary goal of this retrospective study is to understand how the COVID-19 pandemic differentially impacted transplant status across race, sex, age, primary insurance, and geographic regions by examining which candidates: (i) remained on the waitlist, (ii) received transplants, or (iii) were removed from the waitlist due to severe sickness or death on a national level. The trend analysis aggregated by monthly transplant data from 1 December 2019 to 31 May 2021 (18 months) at the transplant center level. Ten variables about every transplant candidate were extracted from UNOS standard transplant analysis and research (STAR) data and analyzed. Characteristics of demographical groups were analyzed bivariately using t-test or Mann-Whitney U test for continuous variables and using Chi-sq/Fishers exact tests for categorical variables. The trend analysis with the study period of 18 months included 31,336 transplants across 327 transplant centers. Patients experienced a longer waiting time when their registration centers in a county where high numbers of COVID-19 deaths were observed (SHR < 0.9999, < 0.01). White candidates had a more significant transplant rate reduction than minority candidates (-32.19% vs. -20.15%) while minority candidates were found to have a higher waitlist removal rate than White candidates (9.23% vs. 9.45%). Compared to minority patients, White candidates' sub-distribution hazard ratio of the transplant waiting time was reduced by 55% during the pandemic period. Candidates in the Northwest United States had a more significant reduction in the transplant rate and a greater increase in the removal rate during the pandemic period. Based on this study, waitlist status and disposition varied significantly based on patient sociodemographic factors. During the pandemic period, minority patients, those with public insurance, older patients, and those in counties with high numbers of COVID-19 deaths experienced longer wait times. In contrast, older, White, male, Medicare, and high CPRA patients had a statistically significant higher risk of waitlist removal due to severe sickness or death. The results of this study should be considered carefully as we approach a reopening world post-COVID-19, and further studies should be conducted to elucidate the relationship between transplant candidate sociodemographic status and medical outcomes during this era.
这项回顾性研究的主要目标是,通过调查哪些候选人:(i)仍在等待名单上,(ii)接受了移植,或(iii)在全国范围内因重病或死亡而被从等待名单上移除,来了解新冠疫情对不同种族、性别、年龄、主要保险类型和地理区域的移植状态产生了怎样的不同影响。趋势分析按移植中心层面从2019年12月1日至2021年5月31日(18个月)的月度移植数据进行汇总。从器官共享联合网络(UNOS)标准移植分析与研究(STAR)数据中提取并分析了每位移植候选人的十个变量。使用t检验或Mann-Whitney U检验对连续变量进行双变量分析,以分析人口统计学组的特征;对于分类变量,则使用卡方检验/费舍尔精确检验。为期18个月的趋势分析涵盖了327个移植中心的31336例移植手术。当患者的登记中心所在县新冠死亡人数较多时,患者的等待时间更长(标准化死亡比<0.9999,P<0.01)。白人候选人的移植率下降幅度比少数族裔候选人更大(-32.19%对-20.15%),而少数族裔候选人的等待名单移除率高于白人候选人(9.23%对9.45%)。与少数族裔患者相比,在疫情期间,白人候选人移植等待时间的亚分布风险比降低了55%。在疫情期间,美国西北部的候选人移植率下降幅度更大,移除率上升幅度也更大。基于这项研究,等待名单状态和处置情况因患者的社会人口因素而有显著差异。在疫情期间,少数族裔患者、有公共保险的患者、老年患者以及所在县新冠死亡人数较多的患者等待时间更长。相比之下,年龄较大、白人、男性、享有医疗保险以及器官分配优先排序较高(CPRA)的患者因重病或死亡而被从等待名单上移除的风险在统计学上显著更高。在我们走向新冠疫情后的世界重新开放之际,应仔细考虑这项研究的结果,并且应开展进一步研究以阐明这一时期移植候选人社会人口状况与医疗结果之间的关系。