Department of Nephrology, Cliniques Universitaires Saint-Luc, Institute of Experimental and Clinical Research, Université Catholique de Louvain, Brussels, Belgium.
Department of Nephrology, Centre Hospitalier Universitaire Amiens-Picardie, Amiens, France.
Nephrol Dial Transplant. 2021 Nov 9;36(11):2094-2105. doi: 10.1093/ndt/gfab200.
Coronavirus disease 2019 (COVID-19) has exposed haemodialysis (HD) patients and kidney transplant (KT) recipients to an unprecedented life-threatening infectious disease, raising concerns about kidney replacement therapy (KRT) strategy during the pandemic. This study investigated the association of the type of KRT with COVID-19 severity, adjusting for differences in individual characteristics.
Data on KT recipients and HD patients diagnosed with COVID-19 between 1 February 2020 and 1 December 2020 were retrieved from the European Renal Association COVID-19 Database. Cox regression models adjusted for age, sex, frailty and comorbidities were used to estimate hazard ratios (HRs) for 28-day mortality risk in all patients and in the subsets that were tested because of symptoms.
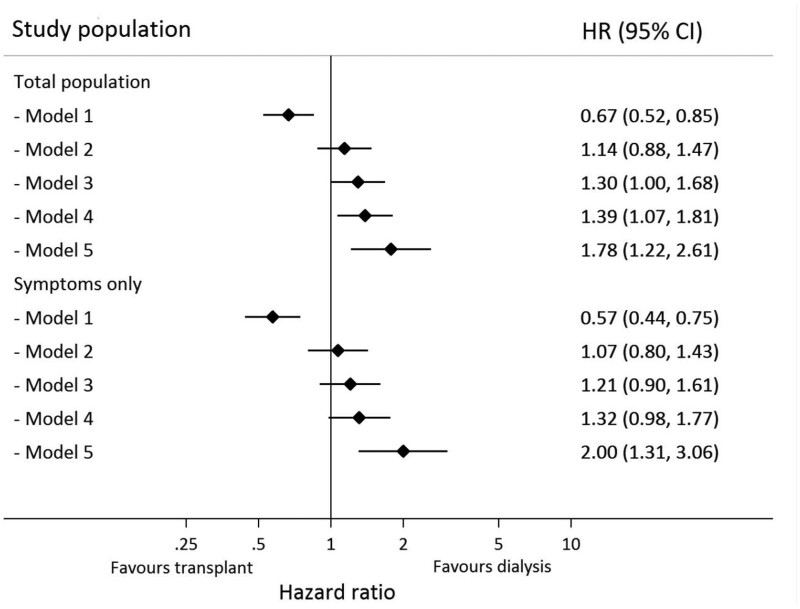
A total of 1670 patients (496 functional KT and 1174 HD) were included; 16.9% of KT and 23.9% of HD patients died within 28 days of presentation. The unadjusted 28-day mortality risk was 33% lower in KT recipients compared with HD patients {HR 0.67 [95% confidence interval (CI) 0.52-0.85]}. In a fully adjusted model, the risk was 78% higher in KT recipients [HR 1.78 (95% CI 1.22-2.61)] compared with HD patients. This association was similar in patients tested because of symptoms [fully adjusted model HR 2.00 (95% CI 1.31-3.06)]. This risk was dramatically increased during the first post-transplant year. Results were similar for other endpoints (e.g. hospitalization, intensive care unit admission and mortality >28 days) and across subgroups.
KT recipients had a greater risk of a more severe course of COVID-19 compared with HD patients, therefore they require specific infection mitigation strategies.
2019 年冠状病毒病(COVID-19)使血液透析(HD)患者和肾移植(KT)受者面临前所未有的危及生命的传染病,这引发了人们对大流行期间肾脏替代治疗(KRT)策略的关注。本研究调查了 KRT 类型与 COVID-19 严重程度之间的关联,并对个体特征的差异进行了调整。
从欧洲肾脏协会 COVID-19 数据库中检索了 2020 年 2 月 1 日至 2020 年 12 月 1 日期间被诊断患有 COVID-19 的 KT 受者和 HD 患者的数据。使用 Cox 回归模型,根据年龄、性别、虚弱和合并症对所有患者以及因症状而接受检测的患者亚组进行调整,以估计 28 天死亡率风险的危险比(HR)。
共纳入 1670 例患者(496 例功能性 KT 和 1174 例 HD);16.9%的 KT 和 23.9%的 HD 患者在出现症状后的 28 天内死亡。与 HD 患者相比,KT 受者未经调整的 28 天死亡率风险低 33%[HR 0.67(95%置信区间 0.52-0.85)]。在完全调整的模型中,KT 受者的风险比 HD 患者高 78%[HR 1.78(95%置信区间 1.22-2.61)]。在因症状而接受检测的患者中,这种关联相似[完全调整模型 HR 2.00(95%置信区间 1.31-3.06)]。这种风险在移植后的第一年急剧增加。其他终点(如住院、重症监护病房入院和 28 天后死亡率)和亚组的结果相似。
与 HD 患者相比,KT 受者 COVID-19 病程更严重的风险更高,因此他们需要特定的感染缓解策略。